How should individuals with positive T1D autoantibodies be monitored over time?
Individuals who screen positive for ≥1 autoimmune islet cell antibodies need periodic medical monitoring, which includes regular assessments of blood glucose and HbA1c levels. You can also educate them about symptoms of diabetes, diabetic ketoacidosis (DKA), and provide psychosocial support to prepare them for a possible clinical diagnosis for type 1 diabetes (T1D).1

Key Takeaway
Metabolic monitoring in individuals who screened positive for ≥2 T1D autoantibodies to track progression of T1D1
Primary purpose of monitoring is to potentially lower the risk of DKA at Stage 3 T1D diagnosis1
Latest consensus guidance* recommends metabolic monitoring by choosing from multiple available tools, such as OGTT, random blood glucose checks, CGM, HbA1c testing, and SMBG.1
Monitor early-stage T1D in primary care if the required skills and resources are available; refer to specialists upon onset of glucose abnormalities.1
*Consensus report endorsed by EASD, ADA, AACE, ACD, ADCES, ADS, ISPAD, ATTD, DiaUnion, the Endocrine Society and JDRF International.
What are the next steps for individuals who test positive for T1D autoantibodies?
A positive screening for presence of ≥2 T1D antibodies indicate that the individual is in presymptomatic stage of T1D.2 As per the latest consensus guidance, such individuals need metabolic monitoring for the presence of glucose abnormalities, an indicator of disease progression.1,3,4
Presence of dysglycaemia, (fasting plasma glucose ≥100 mg/dL [≥5.6 mmol/L], 2-hour plasma glucose with 75 gm OGTT ≥140 mg/dL [≥7.8 mmol/L], 30/60/90 min glucose ≥200 mg/dL [≥11.1 mmol/L], and/or HbA1c ≥5.7% [≥39 mmol/mol]), in individuals who test positive for ≥2 T1D antibodies indicate Stage 2 T1D.3 Individuals in this stage have a 100% risk of progressing to symptomatic Stage 3 T1D within the next 15 years.2 At this stage (Stage 2) you can provide such individuals and their caregivers the relevant disease-related education and psychosocial support needed to prepare for a possible Stage 3 T1D diagnosis.4,5
What is the purpose of monitoring T1D autoantibodies and glycaemia?
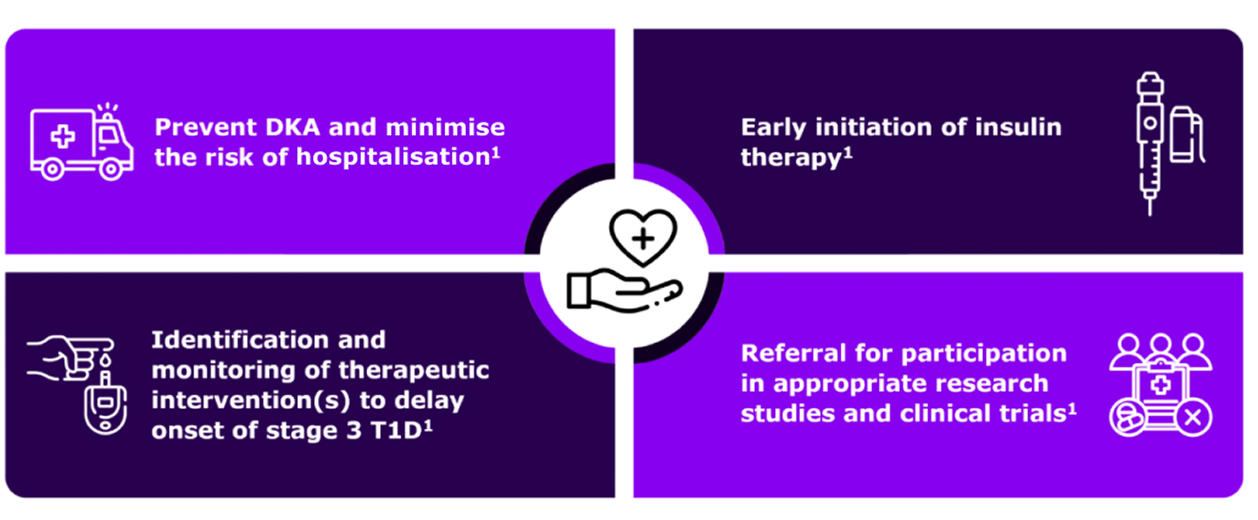
The primary purpose of monitoring individuals with positive screening results for T1D antibodies is to potentially lower the risk of diabetic ketoacidosis (DKA) at Stage 3 T1D diagnosis.1 DKA is a life-threatening condition which is associated with need for hospital admission and potential long-term complications.1 A lower risk of DKA is associated with lower incidence of severe hypoglycaemic events within 10 years post diagnosis.1 Regular medical monitoring, including monitoring glucose abnormalities, will help identify disease progression early on.1,4
Timely monitoring that helps in the early detection of Stage 3 T1D can enable you to promptly initiate early insulin therapy which will help to optimise HbA1c and potentially avoid long-term consequences of prolonged hyperglycaemia.1 Monitoring further avoids misdiagnosis of type 2 diabetes and delay in treatment, and also it may increase patient referrals to clinical trials where appropriate.1
Should you follow specific algorithms and tools to monitor individuals who test positive for T1D autoantibodies?
Monitoring of individuals who screened positive for islet autoantibodies can be largely divided into the two categories:
- Repeat antibody testing: Once an individual tests positive, the second confirmatory test should be done within 3 months.1 A persistent presence of >1 autoantibody indicates presymptomatic Stage 1 T1D.1 Repeat periodic assessments confirming presence of ≥2 autoantibodies along with onset of dysglycaemia indicates progression of disease to Stage 2 T1D.1
- Metabolic monitoring: Choose from multiple available tools, such as regular oral glucose tolerance test (OGTT), random venous or capillary blood glucose, continuous glucose monitoring (CGM), HbA1c testing or self-monitoring of blood glucose (SMBG).1 Testing C-peptide can help you assess measure of beta-cell function and distinguish stages of T1D.1
A detailed description of the methods used for metabolic monitoring is provided in the table below.
| Metric | Pros | Cons | Information gained |
| Oral glucose tolerance test
(OGTT)4 |
|
|
|
| Random venous glucose⁴,⁶ |
|
|
|
| HbA1c⁴ |
|
|
|
| Continuous Glucose Monitoring (CGM) |
|
|
|
| Self monitoring blood glucose (SMBG)⁴ |
|
|
|
At any point of monitoring if you observe onset of hyperglycaemia along with other clinical symptoms such as polyuria, polydipsia, weight loss, fatigue, hunger, blurry vision, and diabetic ketoacidosis (DKA), it indicates disease progression to symptomatic Stage 3 T1D.1
The consensus guidance published in June 2024 provides a detailed algorithm for monitoring of individuals who have been screened positive for islet autoantibodies.1 Below figure illustrates an algorithm for monitoring of people screened positive for ≥2 islet autoantibodies.1
Decision path for monitoring of individuals screened positive for ≥1 islet autoantibodies1
_Decision%20Path%20Video.2026-04-18-11-36-18.png)
Adapted from Phillip M, Achenbach P, Addala A, et al. Consensus guidance for monitoring individuals with islet autoantibody-positive pre-stage 3 type 1 diabetes. Diabetologia. Published online June 24, 2024.
*Monitoring frequency and methodology depends on age, length of time since first detection of islet autoantibody, number of islet autoantibodies detected and presence of symptoms of type 1 diabetes.
Ab, antibody; GP, general practitioner; PRN, pro re nata (as needed); Sx, symptoms; T1D, type 1 diabetes
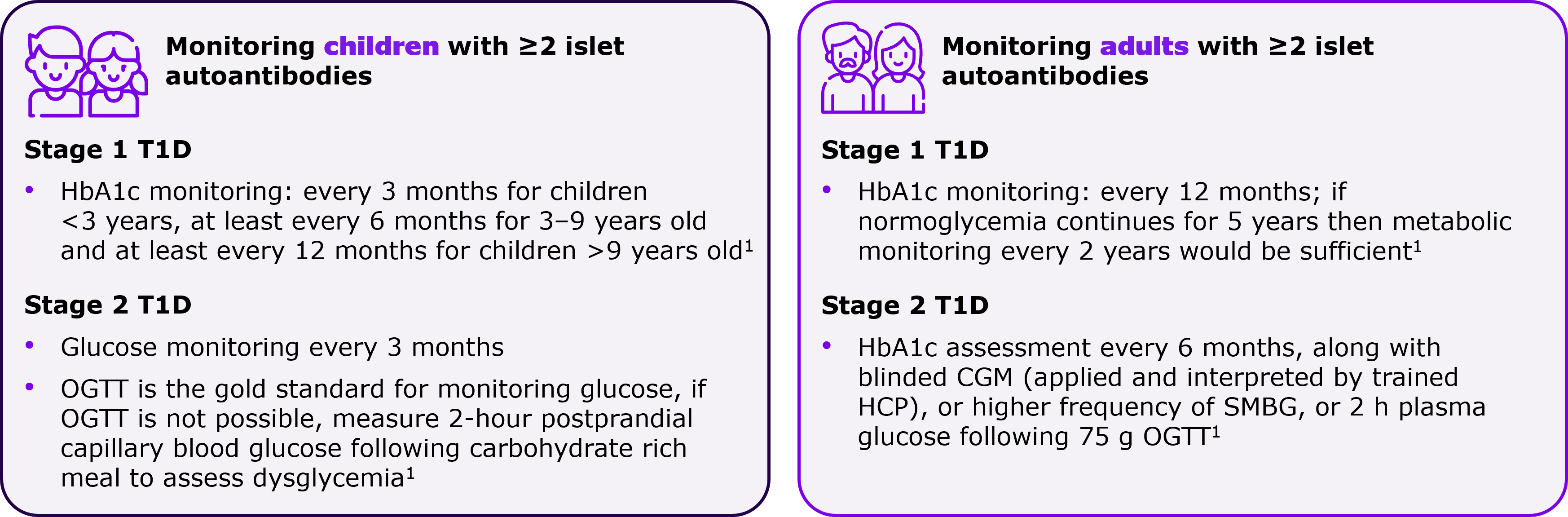
Are there any differences in metabolic monitoring approach in children versus adults?
Progression of T1D among islet autoantibody-positive adults is slower than children, which is why there are minor variations in monitoring approaches.1 You can follow a more frequent metabolic monitoring for children compared to adults.1 Also, children who have progressed to Stage 2 T1D need to be followed up in a specialty care setting.1 Refer to the figure below for more details.
Where should the monitoring be conducted?
Monitoring should be conducted wherever there are the necessary skills and resources to perform the required tests. Early stage (Stage 1 T1D) monitoring can be done in primary-care setting. As soon as you observe indicators of progression of disease to Stage 2 T1D i.e. onset of glucose abnormalities, consider referring to specialty care provider.1
Monitoring individuals who test positive for T1D antibodies is crucial to reduce the risk of DKA and minimise the need for emergency care and hospitalisation1 |
21-OH, 21-hydroxylase; ADA, American Diabetes Association; AACE, American Association of Clinical Endocrinology; ACD, Australian Centre for Diabetes; ADCES, Association of Diabetes Care & Education Specialists; ADS, Australian Diabetes Society; ATTD, Advanced Technologies & Treatments for Diabetes; C-peptide, connecting peptide; CGM, continuous glucose monitoring; DKA, diabetic ketoacidosis; EASD, European Association for the Study of Diabetes; EMA, European Medicines Agency; HbA1c, haemoglobin A1c; IAb, islet autoantibodies; ISPAD, International Society for Pediatric and Adolescent Diabetes; JDRF, Juvenile Diabetes Research Foundation; OGTT, oral glucose tolerance test; FPG, fasting plasma glucose; SMBG, self-monitoring of blood glucose; T1D, type 1 diabetes; TTG, transglutaminase.
- Phillip M, Achenbach P, Addala A, et al. Consensus guidance for monitoring individuals with islet autoantibody-positive pre-stage 3 type 1 diabetes. Diabetologia. Published online June 24, 2024. doi:10.1007/s00125-024-06205-5
- Mameli C, Triolo TM, Chiarelli F, Rewers M, Zuccotti G, Simmons KM. Lessons and gaps in the prediction and prevention of type 1 diabetes. Pharmacol Res. 2023;193:106792. doi:10.1016/j.phrs.2023.106792
- Insel RA, Dunne JL, Atkinson MA, et al. Staging presymptomatic type 1 diabetes: a scientific statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care. 2015;38(10):1964-1974. doi:10.2337/dc15-1419
- Besser REJ, Bell KJ, Couper JJ, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Stages of type 1 diabetes in children and adolescents. Pediatr Diabetes. 2022;23(8):1175-1187
- Greenbaum CJ. A Key to T1D Prevention: Screening and Monitoring Relatives as Part of Clinical Care. Diabetes. 2021;70(5):1029-1037. doi:10.2337/db20-1112
- Helminen O, Aspholm S, Pokka T, et al. OGTT and random plasma glucose in the prediction of type 1 diabetes and time to diagnosis. Diabetologia. 2015;58(8):1787-1796.
Waddling-Gait---Robert,-28-year-old-mild-LOPD-patient
Waddling Gait - Robert, 28-year-old mild LOPD patient
Reaching-Overhead---Robert,-28-year-old-mild-LOPD-patient
Reaching Overhead - Robert, 28-year-old mild LOPD patient
Standing-From-Sitting---Robert,-28-year-old-mild-LOPD-patient
Standing From Sitting - Robert, 28-year-old mild LOPD patient
Climbing-Stairs---Robert,-28-year-old-mild-LOPD-patient
Climbing Stairs - Robert, 28-year-old mild LOPD patient
Waddling-Gait---Karen,-18-year-old-moderate-LOPD-patient

Waddling Gait - Karen, 18-year-old moderate LOPD patient
Reaching-Overhead---Karen,-18-year-old-moderate-LOPD-patient

Reaching Overhead - Karen, 18-year-old moderate LOPD patient
Standing-From-Sitting---Karen,-18-year-old-moderate-LOPD-patient

Standing From Sitting - Karen, 18-year-old moderate LOPD patient
Climbing-Stairs---Karen,-18-year-old-moderate-LOPD-patient

Climbing Stairs - Karen, 18-year-old moderate LOPD patient
ASPIRE-ICT-1-23_Harrington_MAT-AU-2302788-1

ASPIRE-ICT-1-23_Kyle-Blakey_MAT-AU-2302789-1

Which-biologic-and-why--When-to-switch-to-another-one-

Waddling-Gait---Brian,-44-year-old-severe-LOPD-patient

Waddling Gait - Brian, 44-year-old severe LOPD patient
Reaching-Overhead---Brian,-44-year-old-severe-LOPD-patient

Reaching Overhead - Brian, 44-year-old severe LOPD patient
Standing-From-Sitting---Brian,-44-year-old-severe-LOPD-patient

Standing From Sitting - Brian, 44-year-old severe LOPD patient
Climbing-Stairs---Brian,-44-year-old-severe-LOPD-patient

Climbing Stairs - Brian, 44-year-old severe LOPD patient
RESP-ICT2_Wark_MAT-AU-2301970
.webp/jcr:content/RESP-ICT2-Wark_400X300%20(1).webp)
RESP-ICT2_Wark_MAT-AU-2301970
RESP-ICT2_Stone_MAT-AU-2301972
.webp/jcr:content/RESP-ICT2-Stone_400X300%20(1).webp)
RESP-ICT2_Stone_MAT-AU-2301972
Remission-in-rheumatology---Dr-Michelle-Tellus
.webp/jcr:content/RESP-ICT2-Tellus_400X300%20(1).webp)
Remission in rheumatology - Dr Michelle Tellus
Pavord_MAT-AU-2300571

Pavord_MAT-AU-2300571
Wark_MAT-AU-2300572

Wark_MAT-AU-2300572
Q-A-Discussion_MAT-AU-2300573

Q&A-Discussion_MAT-AU-2300573
RESP-ICT3_Tellus_MAT-AU-2302033

RESP-ICT3_Tellus_MAT-AU-2302033
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Hew_MAT-AU-2302035

RESP-ICT3_Hew_MAT-AU-2302035
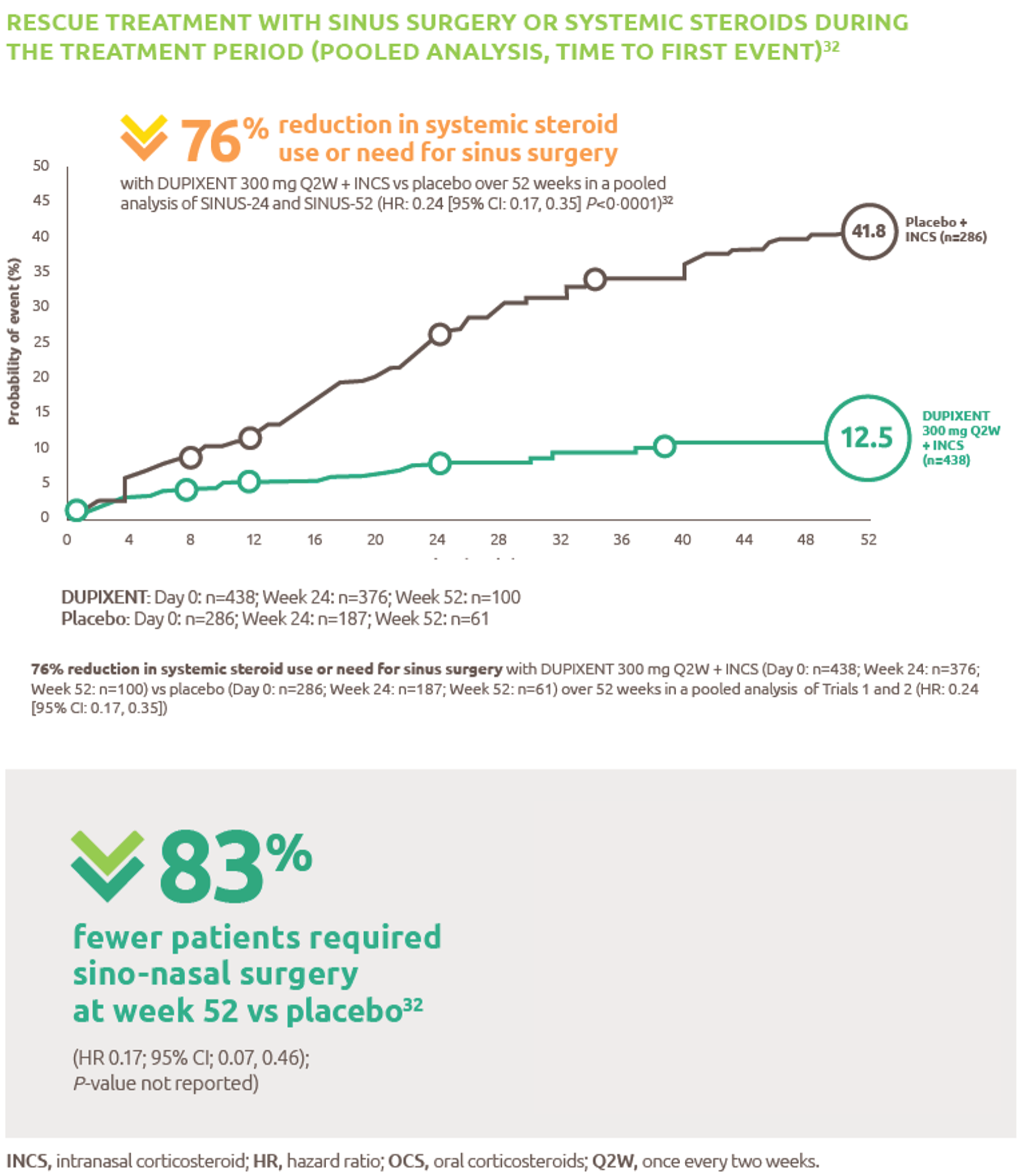
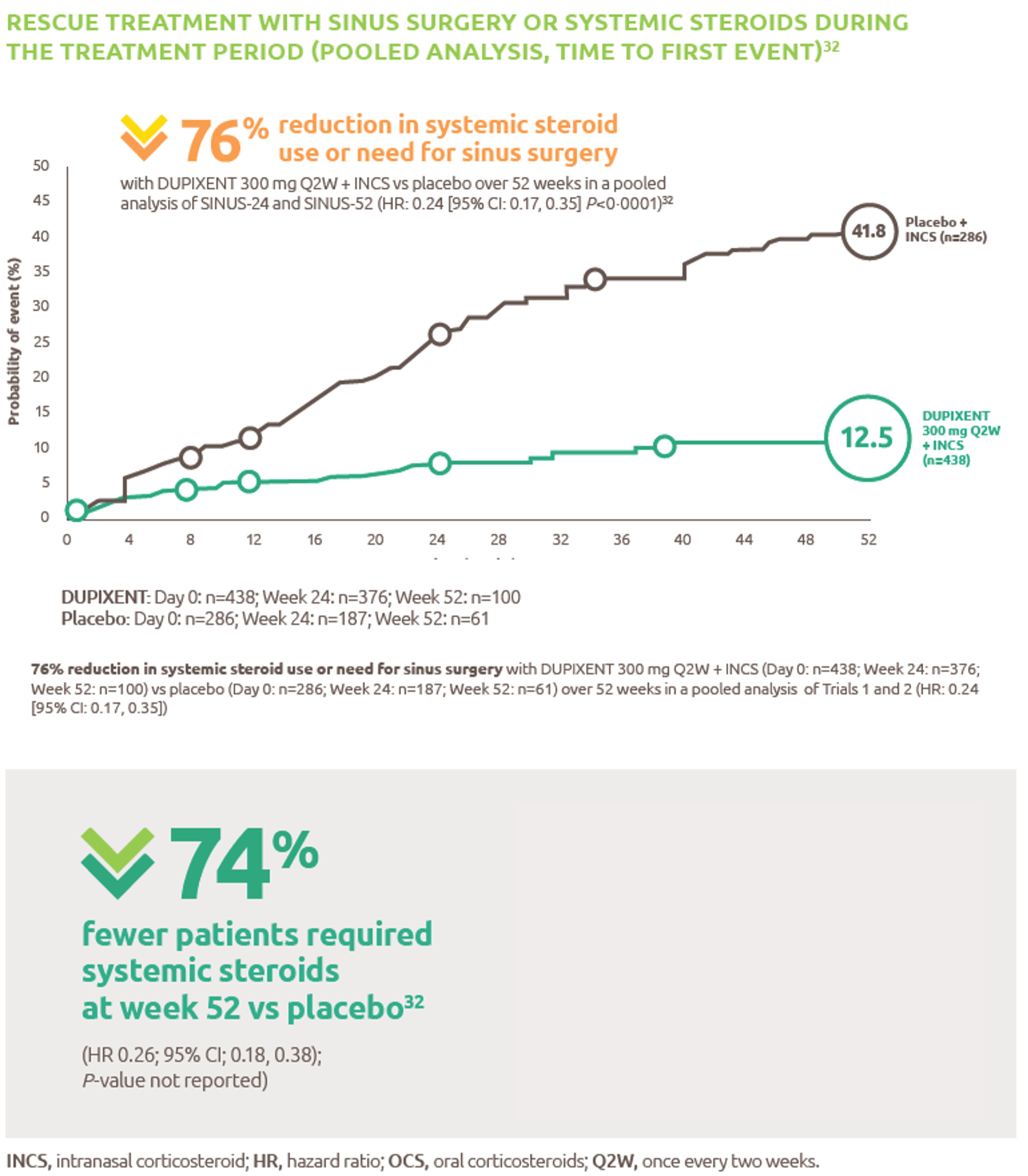
Reduced-need-for-sinus-surgery
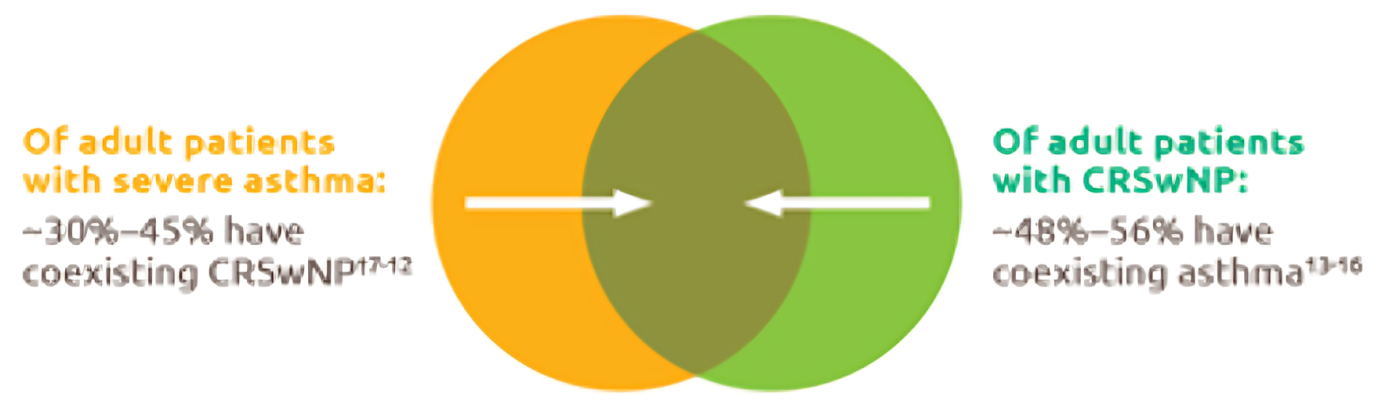
Up-to-45--of-severe-asthma-patients-have-comorbid-CRSwNP
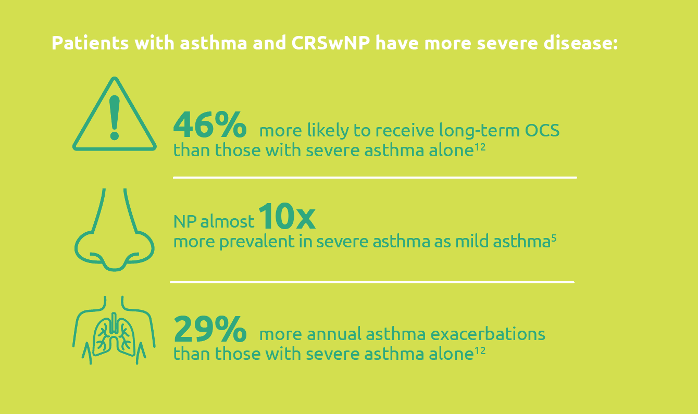
Severe-asthma-with-comorbid-CRSwNP-leads-to-more-severe-disease
.2024-06-04-09-20-31.png)
Less-rescue-oral-corticosteriod-use
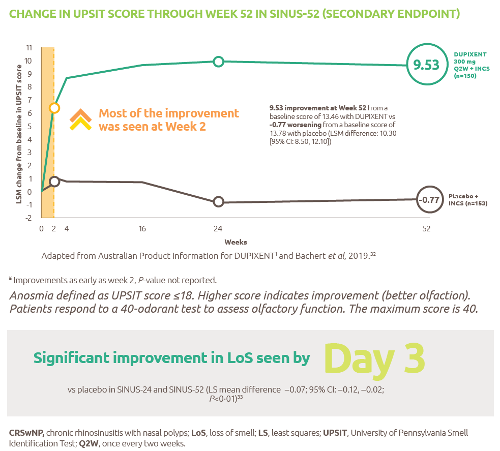
Improved-sense-of-smell
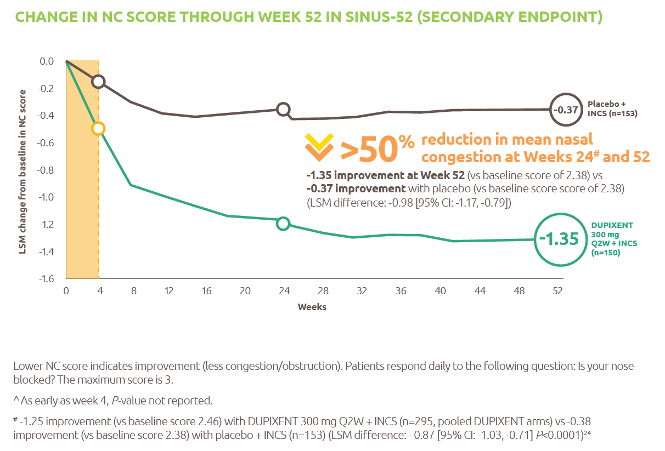
Reduced-obstruction-and-congestion
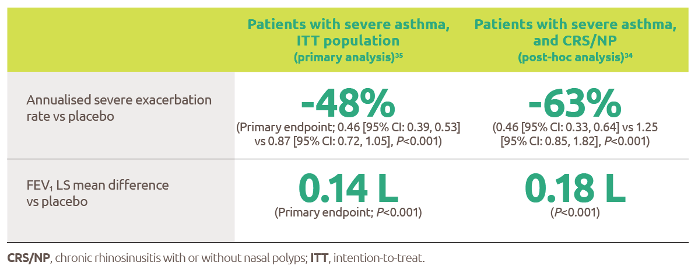
Reduced-asthma-exacerbations-and-improved-lung-function
IL-4-and-IL-13-are-key-and-central-drivers-of-type-2-inflammation

Gaucher-diagnosis-1

RESP-ICT2_Debate_MAT-AU-2301973

RESP-ICT2_Debate_MAT-AU-2301973
RESP-ICT3_Q-A_MAT-AU-2302036

RESP-ICT3_Q&A_MAT-AU-2302036
ASPIRE-ICT1-23_Q-A_MAT-AU-2302791-1

RESP-ICT2_Stone_CS_MAT-AU-2301975

RESP-ICT2_Stone_CS_MAT-AU-2301975
RESP-ICT2_Wark_CS_MAT-AU-2301974

RESP-ICT2_Wark_CS_MAT-AU-2301974
RESP-ICT2_Panel-Discussion_MAT-AU-2301976

RESP-ICT2_Panel-Discussion_MAT-AU-2301976
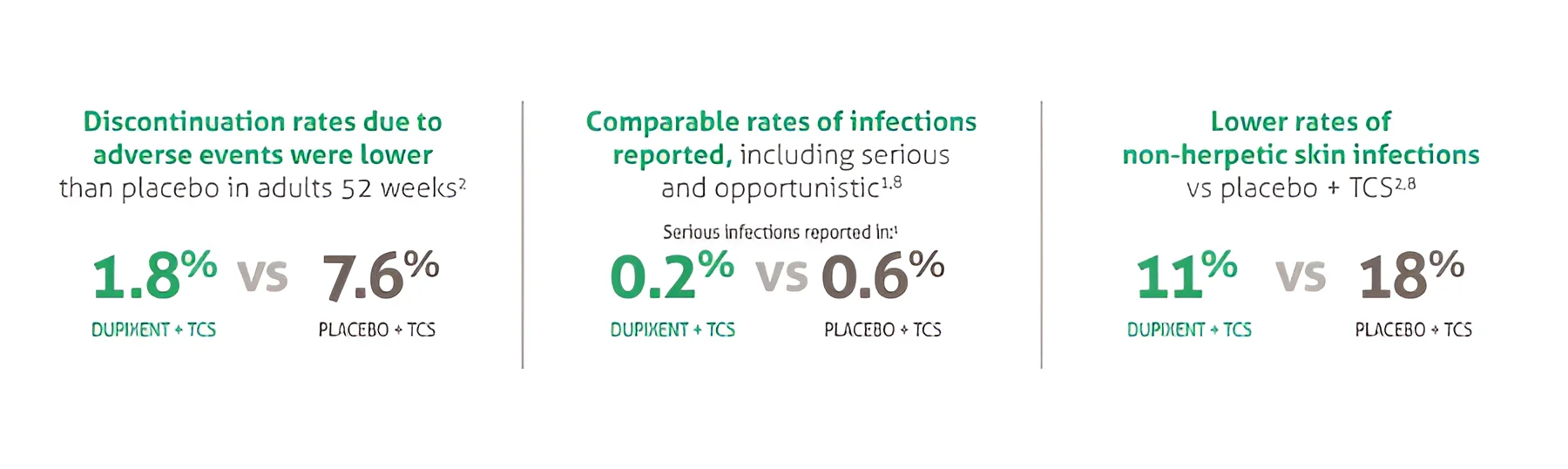
SANA7993_Safety-Page-Tables_V0.2_1_New3
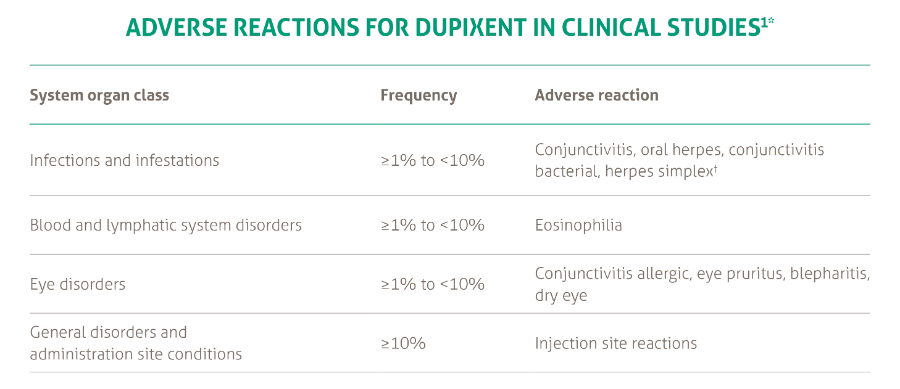
Products_Dermatology_Atopic-Dermatitis_Adverse-Events-Adults_18012021
Le-Cercle---Dr-Christophe-LEFEZ