Venous thromboembolism incidence among patients recommended for pharmacologic thromboembolism prophylaxis after cesarean delivery in selected guidelines
Adapted from Federspiel JJ, et al. J Thromb Haemost. 2021;19:830–838.

Key Takeaway
Incidence of VTE for high-risk caesarean delivery is unclear in the guidelines and risk stratification approaches are widely promulgated. This retrospective cohort study highlights widely different proportions of risk of VTE following delivery across different guidelines in US
Based on the chosen guideline:
- Incidence of pharmacologic recommendation varied from 0.2% (2018 ASH) to 73.4% (2015 RCOG)
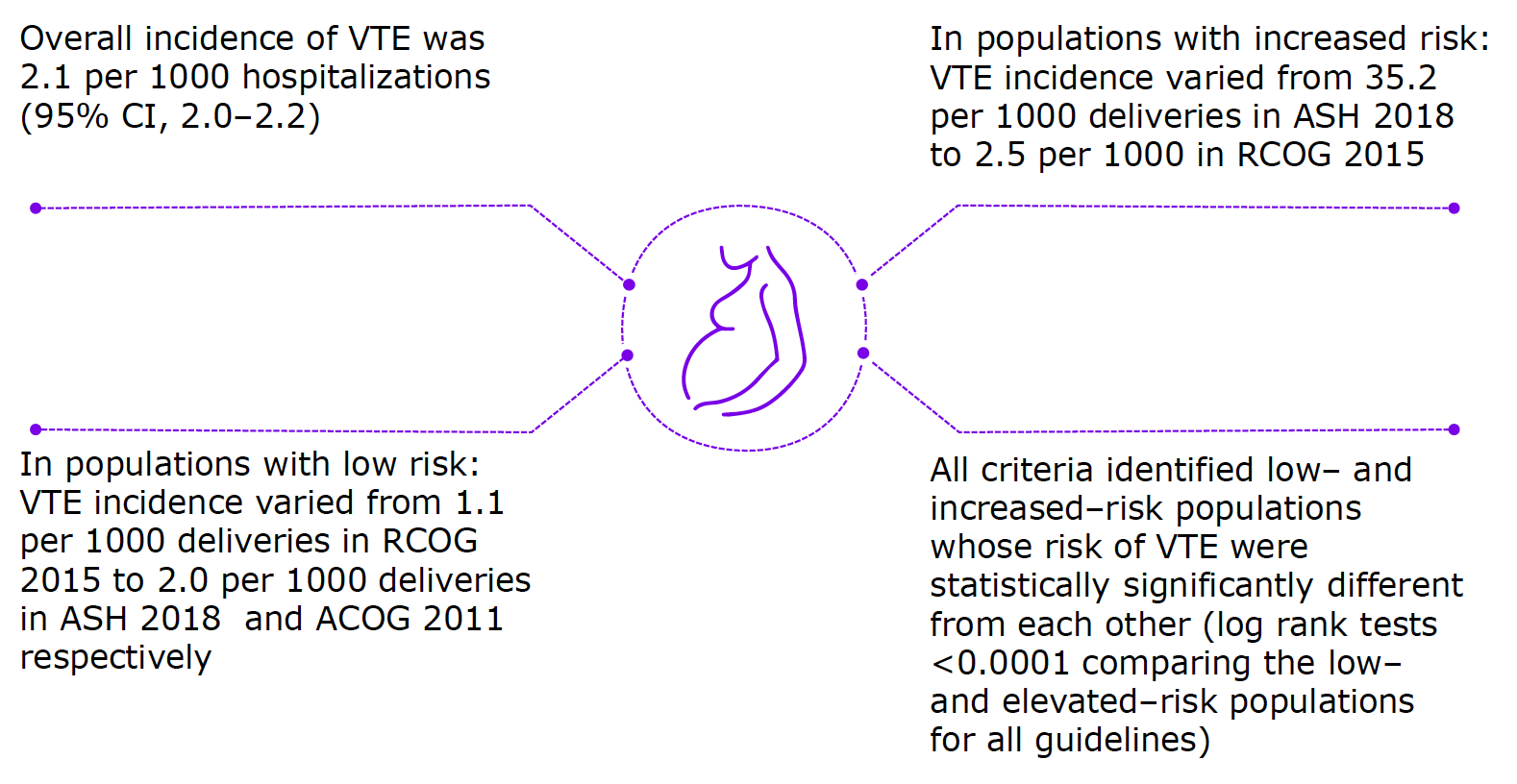
- Incidence of VTE varied from 2.5 (2015 RCOG) to 35.2 (2018 ASH) per 1000 deliveries
Why This Matters
- VTE, particularly PE is a leading cause of pregnancyrelated morbidity and mortality in US and the incidence is increasing
- In the US, it is unknown what drives the implementation of the guidelines identifying the need of pharmacologic prophylaxis after cesarean delivery
- The relationship between the various patient selection criteria for pharmacologic prophylaxis and the subsequent incidence of VTE is unclear

Study Design
To estimate the percentage of cesarean delivery patients for which pharmacologic VTE would be recommended and subsequent incidence of VTE based on selected guidelines: ACOG, RCOG, ACCP, or ASH
Retrospective cohort study
(N = 1,235,149 from 4620 hospitals)
Women who underwent cesarean delivery and were recommended for pharmacologic prophylaxis according to guidelines were included
Outcomes:
- Incidence of VTE among patients recommended for pharmacologic prophylaxis
- Length of stay, inpatient charges, and discharge disposition
October 2015–December 2017
Nationwide Readmissions Database, Healthcare Cost and Utilization project, Agency for Healthcare Research and Quality
- Diagnosis and procedure codes* were used to identify patients undergoing cesarean delivery, the incidence of VTE, and risk factors used to stratify risk in the existing guidelines
- Time–to–event analysis was used to analyze data, stratified by risk categorization in ACOG 2011, ACCP 2012, RCOG 2015, and ASH 2018 guidelines
Key Highlights
- Patients (N = 1,235,149) had a mean age of 29.8 years and the mean length of stay for the hospitalizations was 3.5 days
- Patients requiring pharmacologic prophylaxis
ACOG 2011–0.3%
ASH 2018-0.2%
ACCP 2012–16.2%
RCOG 2015–73.4%
The criteria which yielded biggest difference in VTE risk between low and high-risk patients
![]()
ACOG 2011 (RR: 15.7; 95% CI, 11.7–19.9)
ASH 2018 (RR: 17.3; 95% CI, 12.3–22.2)
ACCP 2012 (RR: 3.9; 95% CI, 3.4–4.3)
RCOG 2015 (RR: 2.2; 95% CI, 1.9–2.5)
Large sample size and data designed to be representative of the US population is the strength of this stud
Limitations
- Retrospective study design
- Use of administrative (billing) data, which may lead to inaccuracies, missing information, code complications or measurement errors
- Any VTE identified and managed solely on an outpatient basis would be excluded
*Performance of cesarean delivery was identified using ICD–10–CM procedure codes 10D00Z0, 10D00Z1, and 10D00Z2
ABBREVIATIONS
ACCP, American College of Chest Physicians; ACOG, American College of Obstetricians and Gynecologists; ASH, American Society of Hematology; CI, confidence interval; PE, pulmonary embolism; RCOG, Royal College of Obstetricians and Gynaecologists; RR, relative risk; VTE, venous thromboembolism; US, United States.
Federspiel JJ, Wein LE, Addae–Konadu KL, et al. Venous thromboembolism incidence among patients recommended for pharmacologic thromboembolism prophylaxis after cesarean delivery in selected guidelines. J Thromb Haemost. 2021;19:830–838. DOI: 10.1111/jth.15218
MAT-BH-2300436/V1/June2023