Economic Burden of COPD in KSA

Chronic Obstructive Pulmonary Disease (COPD) is a progressive lung condition characterized by breathing difficulties, with significant impacts on patients' quality of life.
Global Impact
Global Death Toll:
- Globally, COPD is the third leading cause of death, following ischemic heart disease and stroke1
- In 2019 alone, it caused 3.23 Million deaths worldwide, representing 6% of total global deaths1,2.
Widespread Prevalence:
- Approximately 299.4 Million cases were reported globally in 2017, showing a 24% increase since 20073.
- The prevalence of COPD is projected to increase, with an estimated 5.4 Million deaths by 20604.
DALYs:
- COPD accounts for the majority of Disability-Adjusted Life Years (DALYs) among chronic respiratory diseases5, causing 2.6% of global DALYs in 20156.
COPD Burden in Kingdom of Saudi Arabia
COPD presents a significant health challenge with rising prevalence rates and economic impact:
-
COPD prevalence increased by 49% from 1990 to 2019, with 2,053 cases per 100,000 people reported in 20197.
-
Mortality Impact: COPD accounts for about 1.65% of all-cause deaths8.
-
Macroeconomic Impact: According to the World Bank, the estimated economic loss attributed to COPD in 2017 was approximately $12.497 Billion, reflecting the long-term economic consequences of unmanaged COPD in the region9.
Costs of Treatment and Care in Kingdom of Saudi Arabia:
Direct Costs:
Healthcare Expenditures: COPD is one of the non-communicable diseases (NCDs) contributing to Saudi Arabia's healthcare expenditures, which amount to SAR 66 Billion annually10.
Hospitalization and Treatment: The direct costs associated with COPD primarily include expenses related to hospitalization and treatment of exacerbations. These costs are significant drivers of healthcare spending11-12.
Indirect Costs
Productivity Losses: The indirect costs of COPD include reduced workforce participation and loss in national productivity due to premature mortality, disability, and workplace losses. These losses are valued at SAR 25.6 Billion annually10.
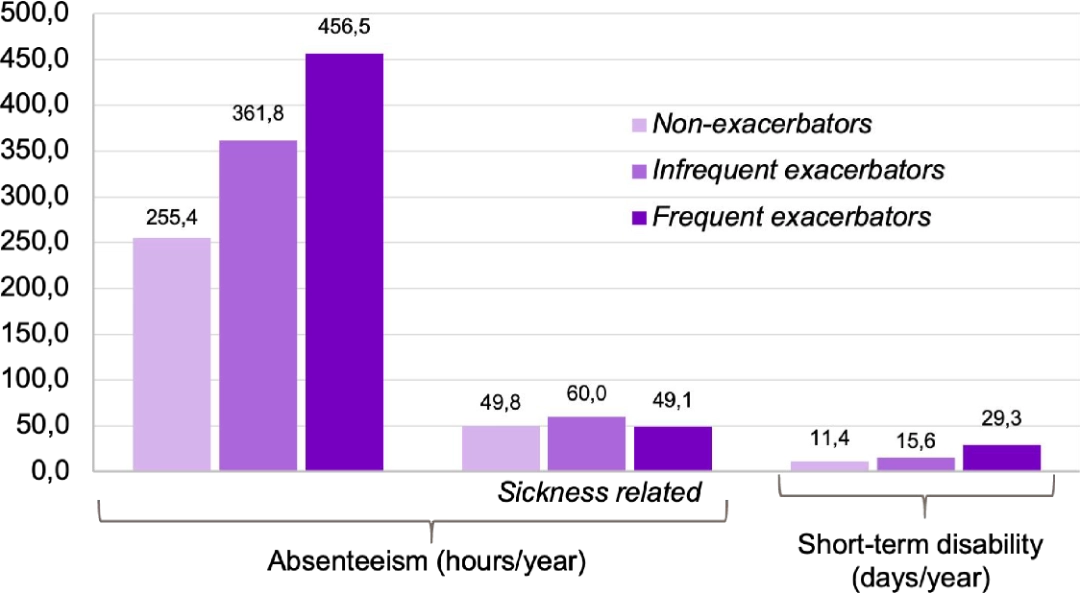
Productivity claims associated with COPD were responsible for 10% of the overall COPD cost burden for working patients13:
Productivity Losses:
- Frequent exacerbators experience the highest productivity loss: 456.5
- Infrequent exacerbators have a significant loss as well: 361.8
- Non-exacerbators show the lowest productivity loss: 255.4
→ Exacerbations directly correlate with increasing productivity losses.
Lost Work Time (sick leave):
- Frequent exacerbators also show the highest amount of lost work time: 60.0
- Non-exacerbators experience less time away from work: 49.8
- Infrequent exacerbators fall in between: 60.0
→ Exacerbations are key drivers of absenteeism in COPD patients.
Decreased Productivity (Presenteeism)
- Frequent exacerbators suffer a higher loss in productivity while at work: 29.3
- Non-exacerbators: 11.4
→ Exacerbations are key drivers of absenteeism in COPD patients.
COPD treatment not only affects productivity of patients, but also of the caregivers:
A Spanish study analyzed the burden borne by informal caregivers (n=220,892) of patients with COPD14.
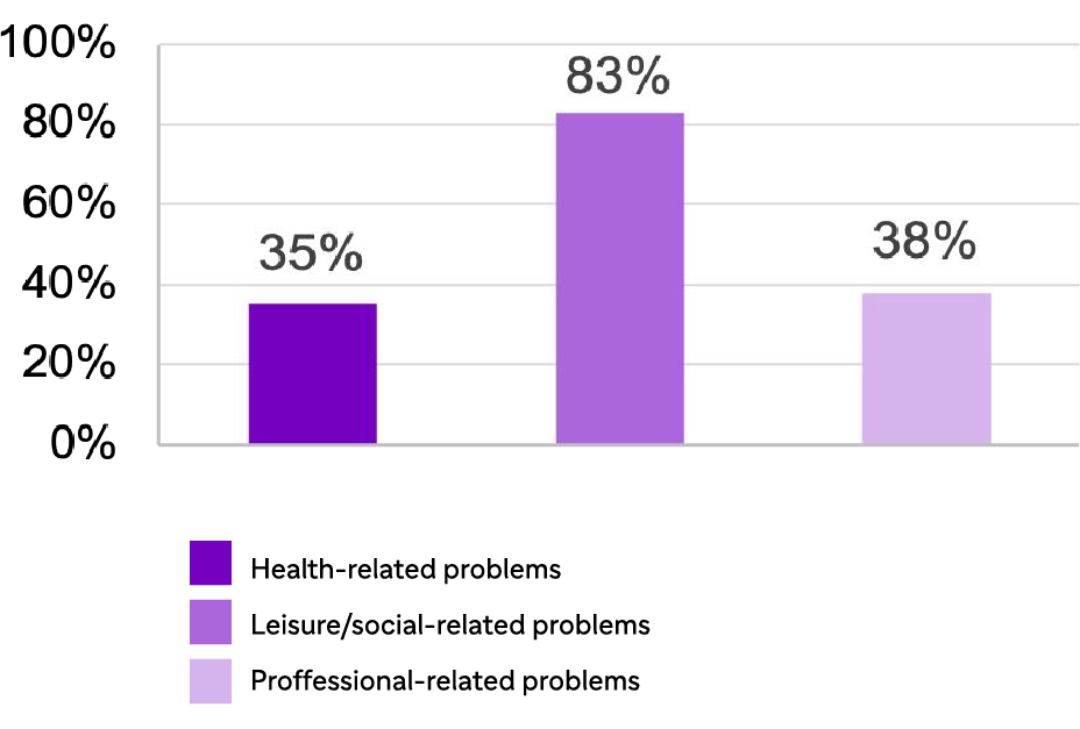
% of informal caregivers (of COPD patients) with health-,
professional-,and leisure/social-related problems
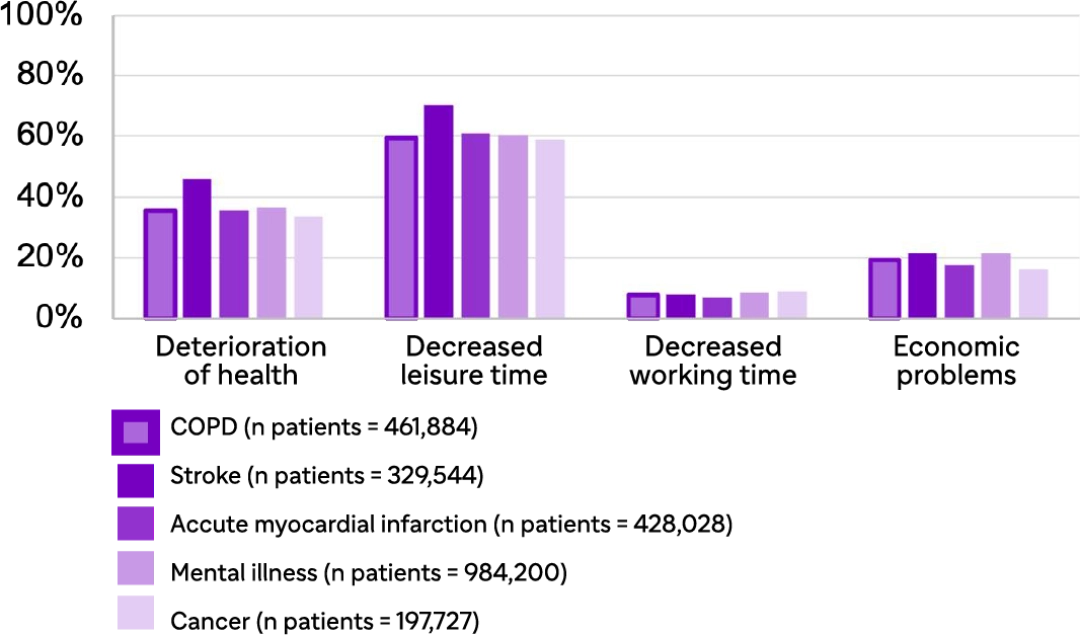
% of informal caregivers of COPD patients having problems
vs. caregivers of patients with other chronic diseases
Caregivers face severe challenges:
- 83% of caregivers report leisure/social-related problems, followed by 38% experiencing professional-related problems and 35% facing health issues.
- COPD caregivers, more than those of other chronic diseases like stroke or myocardial infarction, face greater deterioration of health and a marked decrease in leisure time.
- The comparison with caregivers of other chronic diseases further emphasizes the unique burden COPD imposes, showing higher rates of decreased leisure time and overall strain on caregivers.
- https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death. Published December 2020. Accessed December 2021.
- https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd). Published June 2021. Accessed December 2021.
- GBD 2017 Causes of Death Collaborators. Lancet. 2018;392:1736-1788.
- GOLD. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2022.
- Zou, J., Sun, T., Song, X. et al. Distributions and trends of the global burden of COPD attributable to risk factors by SDI, age, and sex from 1990 to 2019: a systematic analysis of GBD 2019 data. Respir Res 23, 90 (2022). https://doi.org/10.1186/s12931-022-02011-y.
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Lancet. 2018;392:1789-1858.
- 10.1371/journal.pone.0268772
- https://www.liebertpub.com/doi/10.1089/jamp.2023.0016
- https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(23)00217-6/fulltext
- https://www.undp.org/sites/g/files/zskgke326/files/2024-02/ksa_ncd_ic_report_eng.pdf
- https://pmc.ncbi.nlm.nih.gov/articles/PMC6785905/
- https://journaljpri.com/index.php/JPRI/article/view/1321
- Patel G, et al. Int J Chron Obstruct Pulmon Dis. 2018; 13: 2301-2311;
- Miravitlles M, et al. Int J Chron Obstruct Pulmon Dis. 2015; 10: 347-356. Data and information from a study conducted in Spain.

