Renal Outcomes After Switching to Agalsidase Beta: A Single-Center Analysis
Renal Outcomes After Switching to Agalsidase Beta
|
|
|
|
|
|
Study objective (1) |
|
To evaluate within-patient clinical outcomes, primarily renal outcomes, in adult patients with FD who were switched from agalsidase alfa or migalastat to agalsidase beta due to renal inefficacy of primary therapy, defined by:
|
Study design and population (1) |
|
|
|
|
Study endpoints (1) |
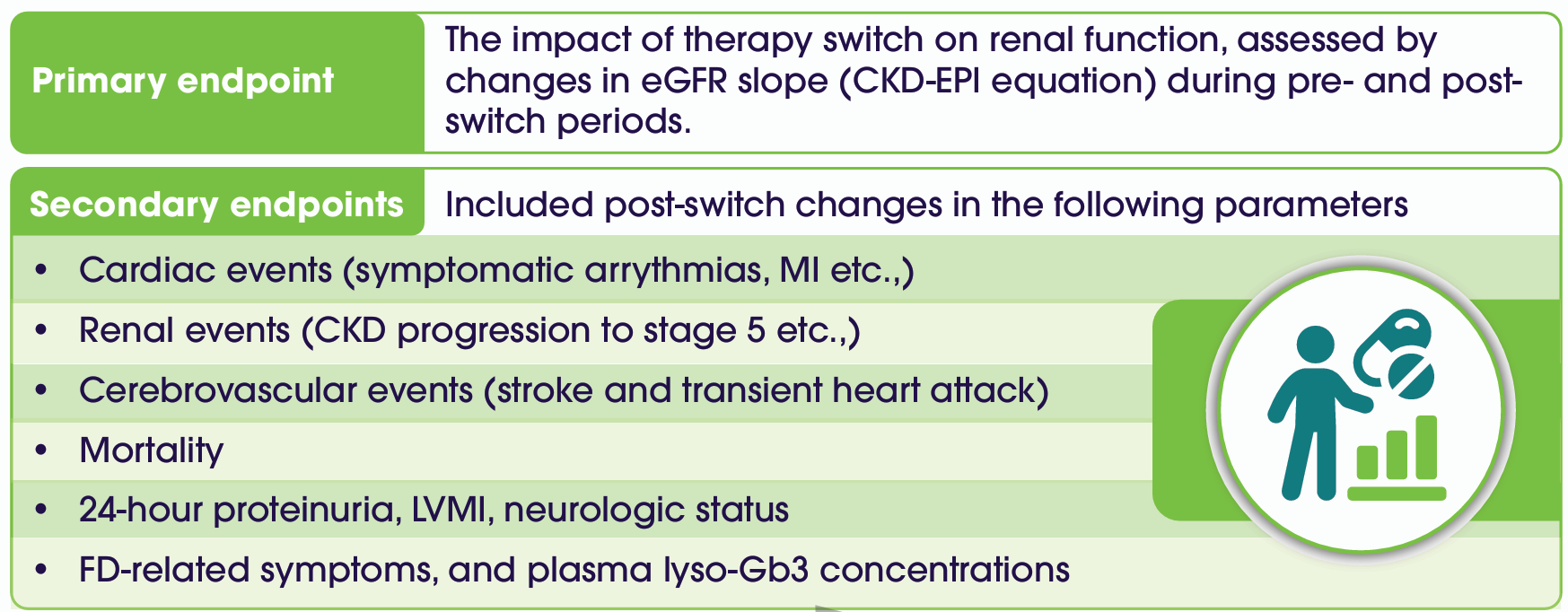
AEs considered were IARs, dyspnoea, hypertension, gastrointestinal symptoms, rigors, temperature change sensation, fever, headache, rhinitis, flushing, and pruritus.
Study result (1) |
|
Parameter comparison across therapy initiation, pre-switch, post-switch visits
|
|||
|
Parameter |
Start of primary
|
Last pre-switch
|
Last post-switch
|
|
eGFR (mL/min/1.73 m²) |
95.5 ± 16.4 |
67.9 ± 20.0* |
67.0 ± 23.6* |
|
Clinical events, n (%) |
0 (0) |
0 (0) |
0 (0) |
|
Proteinuria (mg/day) |
559.1 ± 479.1 |
645.0 ± 1064.4 |
513.6 ± 846.6 |
|
LVMI (g/m²) |
44.3 ± 12.2 |
42.5 ± 12.2 |
513.6 ± 846.6 |
|
Neurologic changes, n (%) |
0 (0) |
1 (9) |
0 (0) |
|
FD-related symptoms, n (%) |
10 (91) |
4 (36)* |
2 (18)* |
|
Adverse events, n (%) |
Not applicable |
2 (18) |
2 (18) |
|
Lyso-Gb3 (ng/mL) |
20.5 ± 17.9 |
8.7 ± 8.1 |
6.9 ± 5.3* |
*Significantly different vs T0 (p<0.05).
Pre and post-switch outcome trajectories
Switching to agalsidase beta stabilized renal function after prior decline, maintained improvements in FD-related symptoms, sustained reductions in lyso-Gb3, and showed comparable safety, with no increase in adverse events post-switch (1). 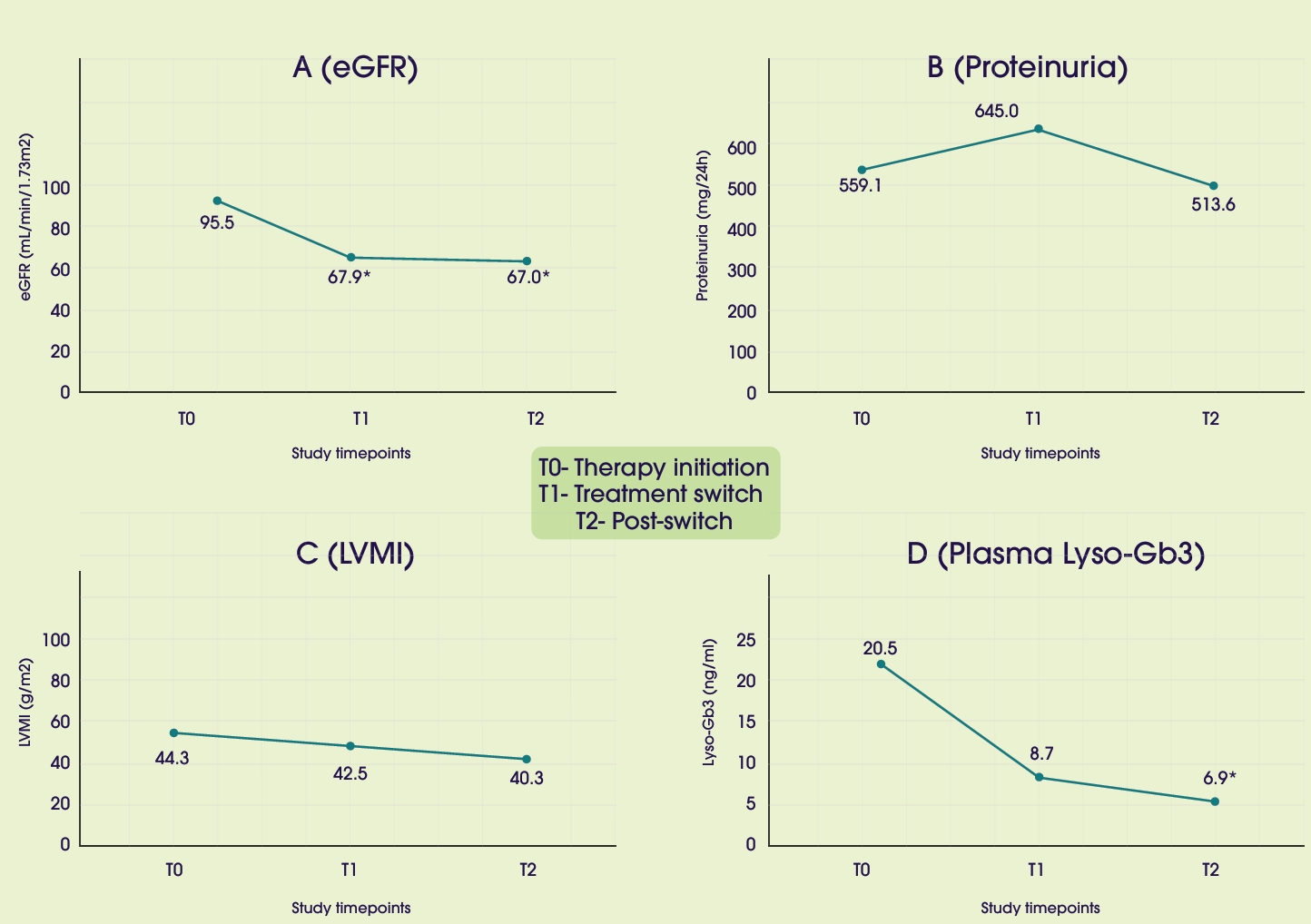
*Significantly different vs T0 (p<0.05).
Fabry-related symptoms and biomarkers:
Most FD-related symptoms improved with primary therapy and remained stable after switching. Plasma lyso-Gb3 levels showed progressive reduction, reaching statistical significance at 24 months versus baseline (p<0.05), although slope differences between treatment periods were not significant (1).
Consistent with these findings, switching to agalsidase beta in patients with progressive renal decline under agalsidase alfa or migalastat resulted in stabilization of eGFR slope, reinforcing the role of dose optimization in ERT to attenuate FD progression and improve renal outcomes (1).
Abbreviation
FD – Fabry disease; Gb3 – Globotriaosylceramide; ERT – Enzyme replacement therapy; eGFR – Estimated glomerular filtration rate; CKD-EPI – Chronic Kidney Disease Epidemiology Collaboration; LVMI – Left ventricular mass index; Lyso-Gb3 – Globotriaosylsphingosine; GLA – α-Galactosidase A; T0 – Start of primary Fabry therapy; T1 – Last pre-switch visit; T2 – Last post-switch visit; AE – Adverse event; IARs – Infusion-related reactions; MI – Myocardial infarction
1. Riccio E, Capuano I, Buonanno P, Iaccarino G, Cirami CL, Mignani R, et al. CLINICAL OUTCOMES IN FABRY PATIENTS SWITCHING TO AGALSIDASE BETA FOR RENAL INEFFECTIVENESS OF THE PRIMARY FABRY THERAPY: A SINGLE-CENTER ANALYSIS.