In-hospital outcomes of ticagrelor versus clopidogrel in the elderly: Results from Improving Care for Cardiovascular Disease in China–Acute Coronary Syndrome project
.svg)
Key takeaway
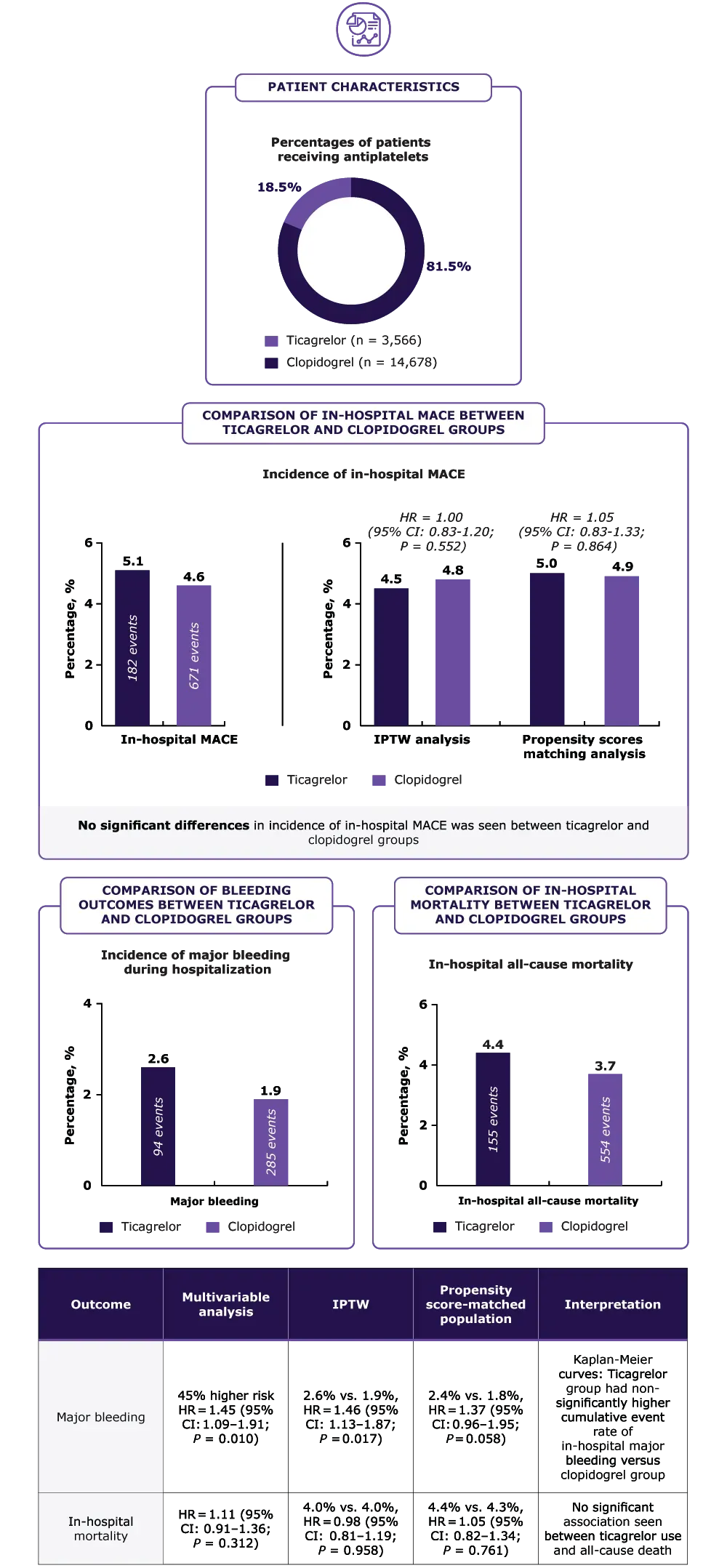
CCC-ACS project, largest study, to compare in-hospital ACS outcomes of elderly patients aged ≥75 years receiving ticagrelor vs clopidogrel during the acute phase highlighted:
- Similar risk of in-hospital MACE
- Higher risk of in-hospital major bleeding with ticagrelor
- Vital preliminary evidence on benefit-risk scenario in elderly patients receiving ticagrelor vs clopidogrel, which is inconsistent with RCT findings and guideline recommendations.
- However, further validation by large pragmatic studies is needed as it may not be feasible to conduct RCTs in this patient population
Why this matters
- Elderly patients ≥75 years constitute a substantial proportion of patients hospitalized for ACS, who are at
- Benefit-risk ratio for antiplatelet drugs may differ between older and younger ACS patients
- Limited evidence exists on the comparative effectiveness and safety of ticagrelor versus clopidogrel in older patients during the acute phase of ACS
Thus, this study compared ticagrelor vs clopidogrel in-hospital outcomes in contemporary
real-world elderly ACS patients aged ≥75 years
Study design
Data obtained from CCC-ACS project, a nationwide registry of AHA and CSC
Inclusion: Hospitalized ACS patients (N = 19,242) aged ≥75 years who received DAPT within 24 hours of first medical contact from November 2014 to December 2019
Exclusion: Patients who received warfarin within 2 weeks before admission (n = 174) and those who switched between ticagrelor and clopidogrel during hospitalization (n = 824)
Patients were divided into two groups: Ticagrelor or clopidogrel
- In-hospital outcomes
- MACEs*
- Major bleeding†
- Any clinically relevant bleeding‡
Results
.webp)
Key limitations
- Although multivariable Cox regression models, IPTW analysis, and propensity score matching analysis were used to adjust for demographics, medical history, and treatment before and during current hospitalization confounders, residual confounding may exist owing to the observational study design.
- All patients included in this study were Chinese, and generalization to non-East Asian patients may necessitate further research.
Please refer source publication Yang N, et al. for additional details.
*MACE defined as composite outcome of cardiac death, re-infarction, and stroke during hospitalization;
†Major bleeding: Any one of the following bleeding events: Fatal bleeding, intracranial bleeding, retroperitoneal bleeding, any bleeding resulting in decline in hemoglobin level of ≥5 g/dL, bleeding requiring surgical intervention or transfusion with overt bleeding;
‡Any clinically relevant bleeding: All documented bleeding events including intracranial bleeding, retroperitoneal bleeding, gastrointestinal bleeding, skin or mucosa bleeding, access-site bleeding and bleeding at other sites, or decline in hemoglobin level of ≥3 g/dL.
ACS, acute coronary syndrome; AHA, American Heart Association; CCS, Improving Care for Cardiovascular Disease in China; CI, confidence interval; CSC, Chinese Society of Cardiology; DAPT, dual antiplatelet therapy; HR, hazard ratio; IPTW, inverse probability of treatment weighting; MACEs, major adverse cardiovascular events; RCT, randomized clinical trial.
- Yang N, Liu J, Liu J, Hao Y, Smith JSC, Huo Y, et al. In-hospital outcomes of ticagrelor versus clopidogrel in patients 75 years or older with acute coronary syndrome: Findings from the Improving Care for Cardiovascular Disease in China (CCC)-Acute Coronary Syndrome Project. Age Ageing. 2022;51(11):afac231. doi: 10.1093/ageing/afac231. PMID: 36413586.
Interested to know more about our products?
.svg)

.svg)
Disclaimer: The images depicted here are fictitious and meant for illustrative purpose only. Any resemblance to any person, living or dead is purely coincidental.





