Approach for patients with coronary artery disease (CAD): focus on LDL-C control

CAD is defined as the pathological process characterised by atherosclerotic plaque accumulation in the epicardial arteries. It covers different conditions, including:1
- Patients with stable angina
- Patients after elective coronary revascularisation procedures, such as percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG)
- Patients with significant coronary disease without prior revascularisation as evidenced by either:
- ≥70% stenosis of at least one coronary artery
- ≥50% stenosis of the left main coronary artery
- Three-vessel obstructive (>70%) disease

Ischaemic heart disease accounts for 16% of all deaths worldwide.2*
The presence of T2DM alongside CAD was shown to increase the risk of a CV event by 28% vs those without diabetes in the CLARIFY study.3
Diabetes is a well-established risk factor for ischaemic heart disease, and CAD accounts for 40–80% of deaths in patients with T2DM.1

New 2024 ESC guidelines for the management of chronic coronary syndromes have been published recently and can be downloaded here
These guidelines present the following steps for management of chronic coronary syndrome (CCS), including CAD4
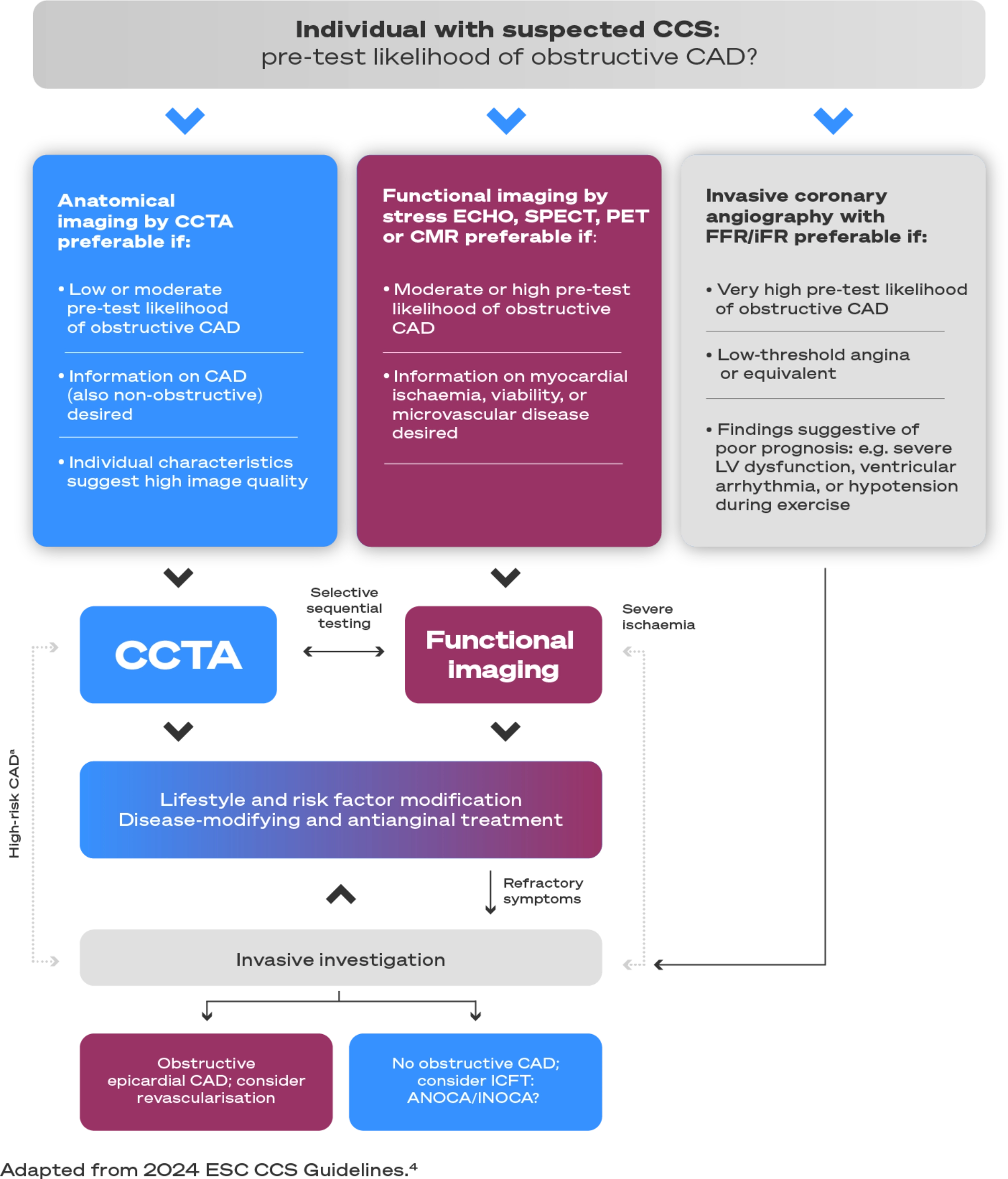
a High–risk CAD: obstructive CAD at high risk of adverse events by CCTA: ≥50% stenosis of the left main stem; three–vessel disease with severe stenoses (≥70% diameter stenosis); single- or two– vessel disease including the proximal LAD with severe stenoses. Consider functional imaging or invasive investigation.
Patients with CAD, with or without T2DM, are at very high CV risk.5 These patients require a holistic multifactorial approach to prevention and management.
Reduce increased levels of causal CV risk factors, such as:5

Target: see below
Target: SBP
120–129 mmHg†

Target is <7.0%
(53 mmol/mol)
Reducing LDL-C levels represents the primary target for reducing CV risk5
According to the 2019 ESC/EAS dyslipidemia guidelines, and 2024 ESC chronic coronary syndromes guidelines, all patients with CAD have the following LDL-C goals.4,5
An LDL-C reduction of ≥50% from baseline‡ and an LDL-C goal of <55 mg/dL (<1.4 mmol/L) are recommended
For patients at very high CV risk (including those with CAD) not achieving their LDL-C goal on a maximum tolerated dose of statin and ezetimibe, combination with a PCSK9i is recommended.5
Recommendations for pharmacological LDL-C lowering5

Step 1
It is recommended that a high-intensity statin is prescribed up to the highest tolerated dose to reach the goals set for the specific level of risk.

Step 2
If the goals are not achieved with the maximum tolerated dose of a statin, combination with ezetimibe is recommended.
Step 3
For secondary prevention, patients at very high risk not achieving their goal on a maximum tolerated dose of a statin and ezetimibe, combination with a PCSK9i is recommended.
Adapted from Vrints et al. 2024 and Mach et al. 20204,5

You should aim to assess your patients response to therapy 6–8 weeks from initiation.5
Prevent The 1st Event for your
CAD patients with or without T2DM¥
*The term stable ischaemic heart disease often is used synonymously with chronic CAD and encompasses a variety of conditions that result in a mismatch between myocardial oxygen supply and demand.6
†Provided the antihypertensive treatment is well tolerated.
‡The term ‘baseline’ refers to the LDL-C level in a person not taking any LDL-C-lowering medication. In people who are taking LDL-C-lowering medication(s), the projected baseline (untreated) LDL-C levels should be estimated, based on the average LDL-C-lowering efficacy of the given medication or combination of medications.5
¥Prevent the first major CV event for your CAD and T2DM patients without prior major CV event.
CLARIFY is an observational registry of patients with chronic coronary syndromes, taking place across 45 countries from 2009 to 2010; follow-up was 5 years. Chronic coronary syndromes were defined by ≥1 of the following criteria: prior myocardial infarction, evidence of coronary stenosis >50%, proven symptomatic myocardial ischaemia, or prior revascularisation procedure.3
ANOCA = angina with non-obstructive coronary arteries; CABG = coronary artery bypass graft; CAD = coronary artery disease; CCS = chronic coronary syndromes; CCTA = coronary computed tomography angiography; CMR = cardiac magnetic resonance; CV = cardiovascular; EAS = European Atherosclerosis Society; ECHO = echocardiography; ESC = European Society of Cardiology; FFR = fractional flow reserve; HbA1c = glycated haemoglobin; ICFT = invasive coronary functional testing; iFR = instantaneous wave-free ratio; INOCA = ischaemia with non-obstructed coronary arteries; LAD = left anterior descending artery; LDL-C = low-density lipoprotein cholesterol; LV = left ventricular; PCI = percutaneous coronary intervention; PCSK9i = proprotein convertase subtilisin/kexin type 9 inhibitor; PET = positron emission tomography; SBP = systolic blood pressure; SPECT = single-photon emission computed tomography; T2DM = type 2 diabetes mellitus.
Referenties
-
Marx N, Federici M, Schütt K, et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes: Developed by the task force on the management of cardiovascular disease in patients with diabetes of the European Society of Cardiology (ESC). Eur Heart J 2023;44(39):4043–4140.
-
World Health Organization. The top 10 causes of death. 2020. Available at: https://www.who.int/ news-room/fact-sheets/detail/the-top-10-causes-of-death. Accessed: August 2024.
-
Mak K, Vidal-Petiot E, Young R, et al. Prevalence of diabetes and impact on cardiovascular events and mortality in patients with chronic coronary syndromes, across multiple geographical regions and ethnicities. Eur J Prev Cardiol. 2021;28:1795–1806.
-
Vrints C, Andreotti F, Koskinas KC, et al. ESC Scientific Document Group. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024:ehae177.
-
Mach F, Baigent C, Catapano AL, et al. ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188.
-
Dababneh E and Goldstein S. Chronic Ischemic Heart Disease Selection of Treatment Modality. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2023.
Bevestig uw status
Bevestig uw status
Sanofi biedt u exclusieve content over onze verschillende therapeutische gebieden op één portal
speciaal voor professionals in de gezondheidszorg, inclusief wetenschappelijk nieuws, een ljst met
evenementen en tools en diensten voor uw dagelijkse praktik.