Rabies
Discover timely medical updates and key resources on preventing and controlling rabies – helping you stay informed and improve patient outcomes.
*Image is not an actual patient.
About rabies
The challenges of rabies
Rabies is an acute viral encephalomyelitis caused by neurotropic viruses of the lyssavirus genus. It is most often transmitted to humans through the bite of an animal infected with rabies.1 In up to 99% of cases, domestic dogs are responsible for rabies virus transmission to humans.
Supporting yellow rabies management through information
Effective management of rabies involves a comprehensive understanding of the condition. For healthcare professionals, staying informed about the disease and evolving patient needs is crucial for providing care.
To foster a broader understanding of rabies, this page offers a range of selected materials and information.
Understanding rabies research and care
Effectively managing rabies requires expertise in its clinical manifestations, vaccination protocols, and emergency care strategies. Here are broad areas of focus in rabies research:
- Implementing case tracking systems in endemic regions to identify at-risk populations
- Administering post‑exposure prophylaxis (vaccine + immunoglobulin) promptly after bites
- Promoting pre‑exposure vaccination for high-risk groups (e.g., veterinarians), plus mass dog vaccination efforts
Don’t miss these key links
Signs and symptoms
Human can be exposed by an animal scratch or bite which has broken the skin, direct contact of the virus with a mucosal surface (eg. nose, eye, mouth) and in rare cases after tissue or organ transplantation from donors who have died with undiagnosed rabies.3
The incubation period for rabies is typically 3-8 weeks, but may vary from 1 week to, on rare occasion, several years. This is dependent upon factors such as the location of virus entry and viral load.3
Initial symptoms of rabies are relatively non-specific including general weakness or discomfort, fever, or headache accompanied by paraesthesia at the wound site.3 As the virus spreads to the central nervous system, progressive and fatal inflammation of the brain and spinal cord develops.2 In the encephalitic phase, manifesting symptoms can include aerophobia, hydrophobia, bizaree behavious, disorientation, hyperactivity.3
Once clinical signs of rabies appear the disease is virtually 100% fatal.2
Virology
There are 14 known species within the genus Lyssavirus, including the classical rabies virus and other closely related lyssaviruses such as the Australian bat lyssavirus and European bat lyssaviruses.4 As the clinical disease caused by classical rabies virus and other lyssaviruses is indistinguishable, the term ‘rabies’ refers to disease caused by any of the known lyssavirus species.3
Diagnosis
No tests are available to diagnose rabies in humans before the onset of clinical disease. In the early stages of disease, saliva and cerebrospinal fluid (CSF) can be tested by virus culture and PCR. Antibody testing can also be performed on CSF. A positive serum antibody test is diagnostic of infection with a lyssavirus in a person who has never been immunised against rabies. Viral shedding in body secretions is intermittent and early tests may be negative for antibodies, therefore repeated testing is often required.4
Prevention
The major source of rabies in humans can be eliminated through ensuring adequate animal vaccination and control. Additional preventative measures include, educating those at risk on bite prevention, appropriate wound management after animal bites and pre-exposure immunisation in high-risk populations.2
Rabies vaccines are available for pre-exposure prophylaxis (PrEP). In an Australian context these are recommended for:3
- People who may receive bites or scratches from bats — these include bat handlers; veterinarians and veterinary nurses; wildlife officers, wildlife carers and zookeepers; wildlife researchers; and others who come into direct contact with bats in any country, including Australia research laboratory workers working with any live lyssavirus people who will be travelling to, or living in, rabies-enzootic areas — give pre-exposure prophylaxis after a risk assessment that considers the likelihood that the person will interact with animals and their access to emergency medical attention
- Travellers to rabies-enzootic regions should be advised to avoid close contact with either wild or domestic animals. This is particularly important for travellers with children. They should be advised about pre-exposure rabies prophylaxis (or, if appropriate, booster doses), and on what to do should they be either bitten or scratched by an animal while abroad. It is recommended that prior to travel, travellers be educated regarding first aid treatment for rabies exposures, irrespective of prior vaccination.3
Epidemiology
The epidemiology of rabies varies depending on the lyssavirus species and the animal host. Lyssaviruses have been found on all continents, except Antarctica.2 Rabies is estimated to cause 59,000 human deaths annually in over 150 countries, with 95% of cases occurring in Africa and Asia. Due to widespread underreporting and uncertain estimates, it is likely that this number is a gross underestimate of the true burden of disease. 99% of rabies cases are dog-mediated and the burden of disease is disproportionally borne by rural poor populations.5
Dog-mediated rabies has been eliminated from Canada, the United States of America, Western Europe, Japan and some Latin American countries.5 Australia, New Zealand, Japan, Papua New Guinea and Pacific Island nations are free from rabies in terrestrial animals.3 There has been a significant reduction in the number of reported cases of dog rabies in Latin America and the Caribbean and bat-mediated rabies now accounts for the majority of lyssavirus cases in this region.5
In some parts of the world, bats are important reservoirs of classical rabies as well as other lyssaviruses such as the Australian bat lyssavirus (ABLV) exclusively found in Australian bats. ABLV was first reported in bats in Australia in 1996; since then, three cases of fatal encephalitis caused by ABLV have been reported in Australians, in 1996, 1998 and 2013.3
Treatment
Post-exposure prophylaxis (PEP) is the immediate treatment of a bite victim after potential rabies exposure. The purpose of PEP is to prevent virus entry into the central nervous system. PEP consists of:
- extensive washing and local treatment of the wound as soon as possible after exposure;
- a course of rabies vaccine that meets WHO standards; and
- the administration of rabies immunoglobulin (RIG), if indicated.
Effective treatment soon after exposure to rabies can prevent the onset of symptoms and death.2
Further post-exposure prophylaxis information can be accessed in the Australian Immunisation Handbook available from https://immunisationhandbook.health.gov.au/vaccine-preventable-diseases/rabies-and-other-lyssaviruses
Featured content

Register to receive full access (Healthcare Professionals Only)
Are you a registered healthcare professional?
Register in less than a minute to access the latest updates and resources to support your practice and help deliver better outcomes for your patients.
-
Rabies. Yellow Book. Centers for Disease Control and Prevention.
https://wwwnc.cdc.gov/travel/yellowbook/2020/travel-related-infectious-diseases/rabies Accessed June 2024 -
Rabies. World Health Organization Fact sheet.
https://www.who.int/en/news-room/fact-sheets/detail/rabies Accessed June 2024 -
Australian Immunisation Handbook 10th edition. Australian Govt. Department of Health. https://immunisationhandbook.health.gov.au/vaccine-preventable-diseases/rabies-and-other-lyssaviruses Accessed June 2024
-
NSW Health. Rabies and other lyssavirus infections (including Australian Bat Lyssavirus) control guidelines. https://www.health.nsw.gov.au/Infectious/controlguideline/Pages/rabies.aspx Access June 2024
-
World Health Organisation. Rabies, Epidemiology and Burden of disease. https://www.who.int/health-topics/rabies/#tab=tab_1 Accessed June 2024
Waddling-Gait---Robert,-28-year-old-mild-LOPD-patient
Waddling Gait - Robert, 28-year-old mild LOPD patient
Reaching-Overhead---Robert,-28-year-old-mild-LOPD-patient
Reaching Overhead - Robert, 28-year-old mild LOPD patient
Standing-From-Sitting---Robert,-28-year-old-mild-LOPD-patient
Standing From Sitting - Robert, 28-year-old mild LOPD patient
Climbing-Stairs---Robert,-28-year-old-mild-LOPD-patient
Climbing Stairs - Robert, 28-year-old mild LOPD patient
Waddling-Gait---Karen,-18-year-old-moderate-LOPD-patient

Waddling Gait - Karen, 18-year-old moderate LOPD patient
Reaching-Overhead---Karen,-18-year-old-moderate-LOPD-patient

Reaching Overhead - Karen, 18-year-old moderate LOPD patient
Standing-From-Sitting---Karen,-18-year-old-moderate-LOPD-patient

Standing From Sitting - Karen, 18-year-old moderate LOPD patient
Climbing-Stairs---Karen,-18-year-old-moderate-LOPD-patient

Climbing Stairs - Karen, 18-year-old moderate LOPD patient
ASPIRE-ICT-1-23_Harrington_MAT-AU-2302788-1

ASPIRE-ICT-1-23_Kyle-Blakey_MAT-AU-2302789-1

Which-biologic-and-why--When-to-switch-to-another-one-

Waddling-Gait---Brian,-44-year-old-severe-LOPD-patient

Waddling Gait - Brian, 44-year-old severe LOPD patient
Reaching-Overhead---Brian,-44-year-old-severe-LOPD-patient

Reaching Overhead - Brian, 44-year-old severe LOPD patient
Standing-From-Sitting---Brian,-44-year-old-severe-LOPD-patient

Standing From Sitting - Brian, 44-year-old severe LOPD patient
Climbing-Stairs---Brian,-44-year-old-severe-LOPD-patient

Climbing Stairs - Brian, 44-year-old severe LOPD patient
RESP-ICT2_Wark_MAT-AU-2301970
.webp/jcr:content/RESP-ICT2-Wark_400X300%20(1).webp)
RESP-ICT2_Wark_MAT-AU-2301970
RESP-ICT2_Stone_MAT-AU-2301972
.webp/jcr:content/RESP-ICT2-Stone_400X300%20(1).webp)
RESP-ICT2_Stone_MAT-AU-2301972
Remission-in-rheumatology---Dr-Michelle-Tellus
.webp/jcr:content/RESP-ICT2-Tellus_400X300%20(1).webp)
Remission in rheumatology - Dr Michelle Tellus
Pavord_MAT-AU-2300571

Pavord_MAT-AU-2300571
Wark_MAT-AU-2300572

Wark_MAT-AU-2300572
Q-A-Discussion_MAT-AU-2300573

Q&A-Discussion_MAT-AU-2300573
RESP-ICT3_Tellus_MAT-AU-2302033

RESP-ICT3_Tellus_MAT-AU-2302033
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Hew_MAT-AU-2302035

RESP-ICT3_Hew_MAT-AU-2302035
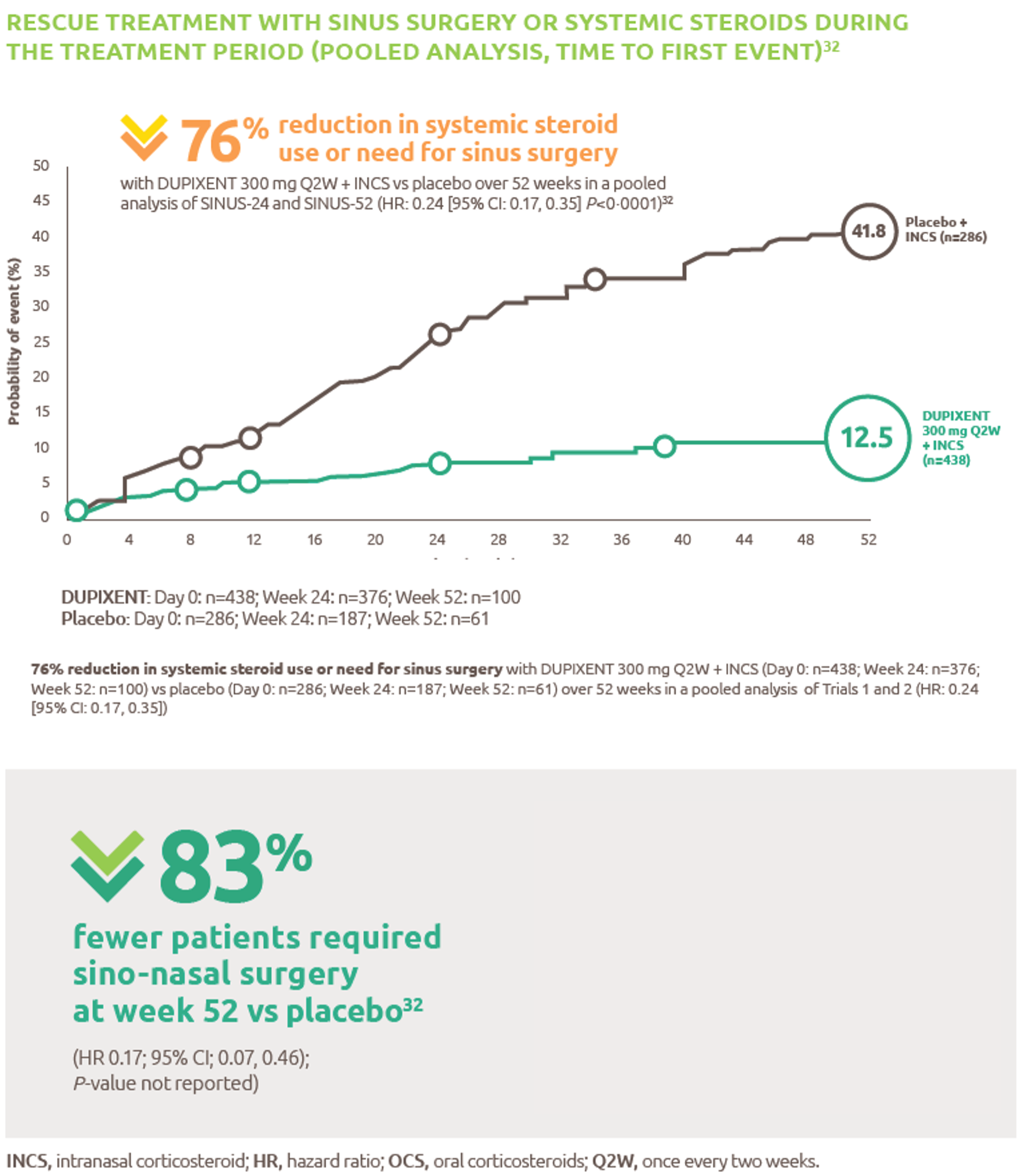
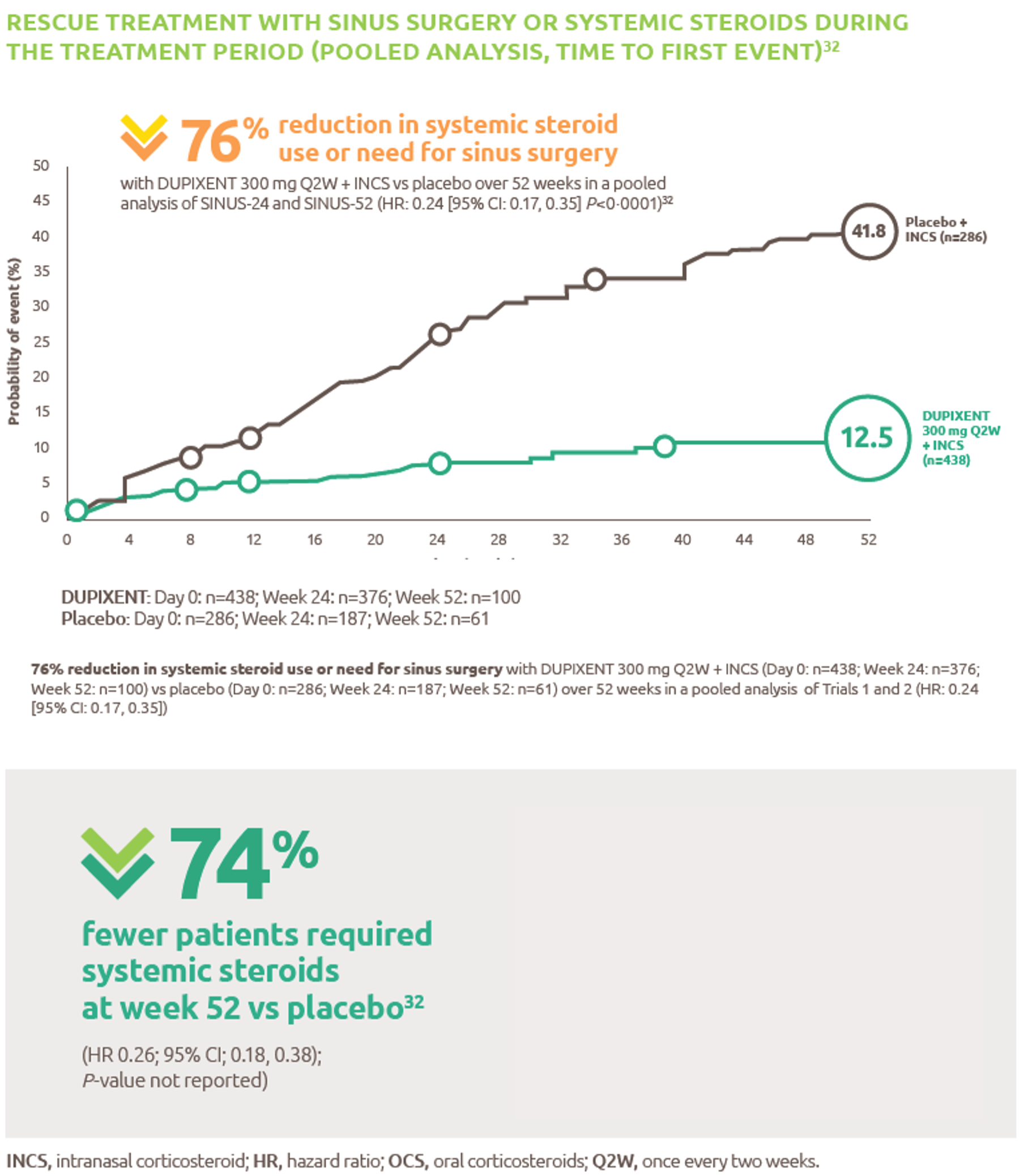
Reduced-need-for-sinus-surgery
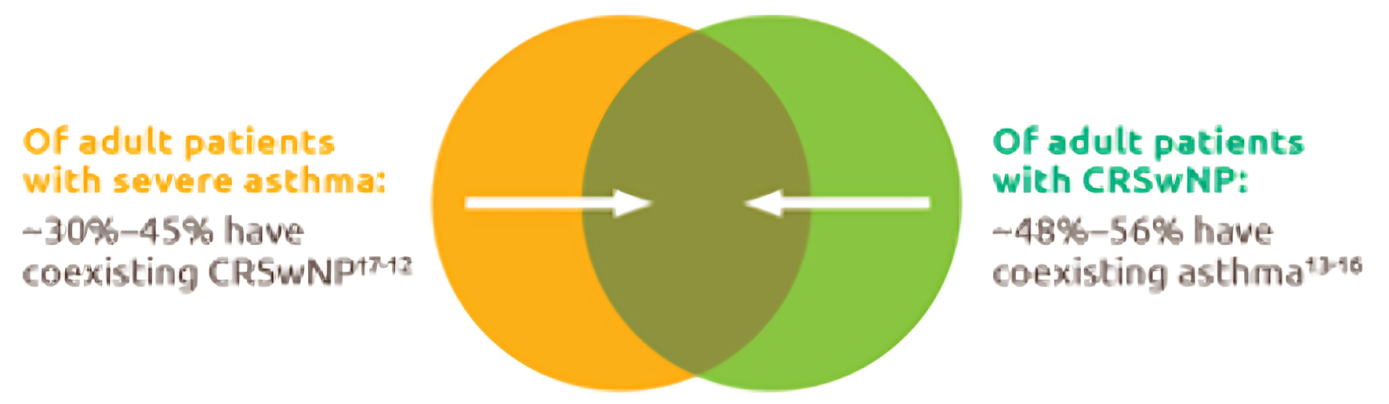
Up-to-45--of-severe-asthma-patients-have-comorbid-CRSwNP
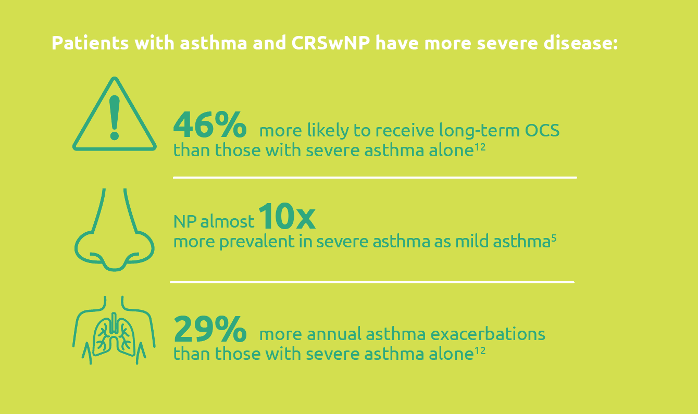
Severe-asthma-with-comorbid-CRSwNP-leads-to-more-severe-disease
.png)
Less-rescue-oral-corticosteriod-use
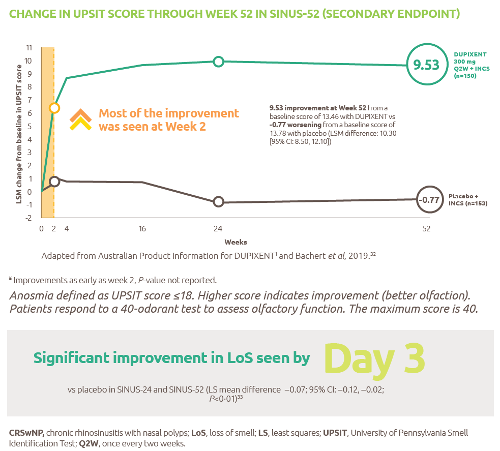
Improved-sense-of-smell
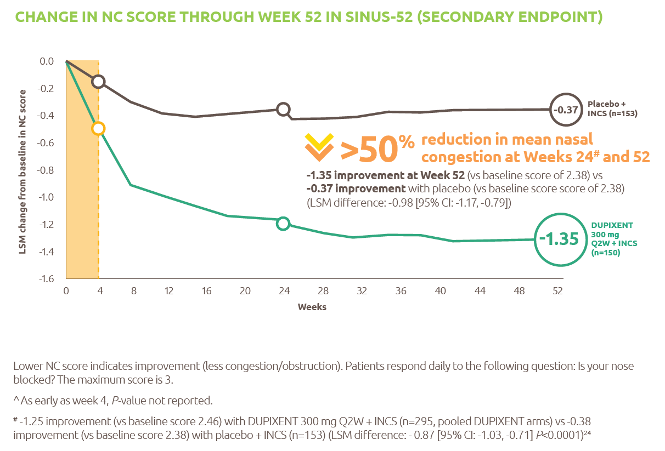
Reduced-obstruction-and-congestion
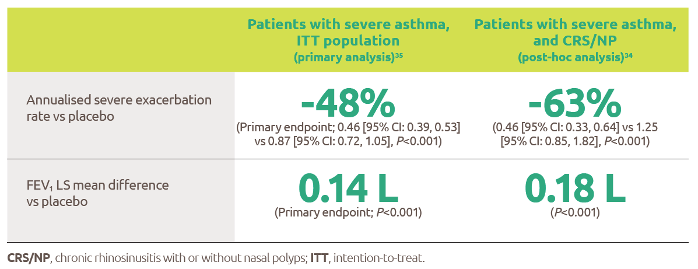
Reduced-asthma-exacerbations-and-improved-lung-function
IL-4-and-IL-13-are-key-and-central-drivers-of-type-2-inflammation

Gaucher-diagnosis-1

RESP-ICT2_Debate_MAT-AU-2301973

RESP-ICT2_Debate_MAT-AU-2301973
RESP-ICT3_Q-A_MAT-AU-2302036

RESP-ICT3_Q&A_MAT-AU-2302036
ASPIRE-ICT1-23_Q-A_MAT-AU-2302791-1

RESP-ICT2_Stone_CS_MAT-AU-2301975

RESP-ICT2_Stone_CS_MAT-AU-2301975
RESP-ICT2_Wark_CS_MAT-AU-2301974

RESP-ICT2_Wark_CS_MAT-AU-2301974
RESP-ICT2_Panel-Discussion_MAT-AU-2301976

RESP-ICT2_Panel-Discussion_MAT-AU-2301976
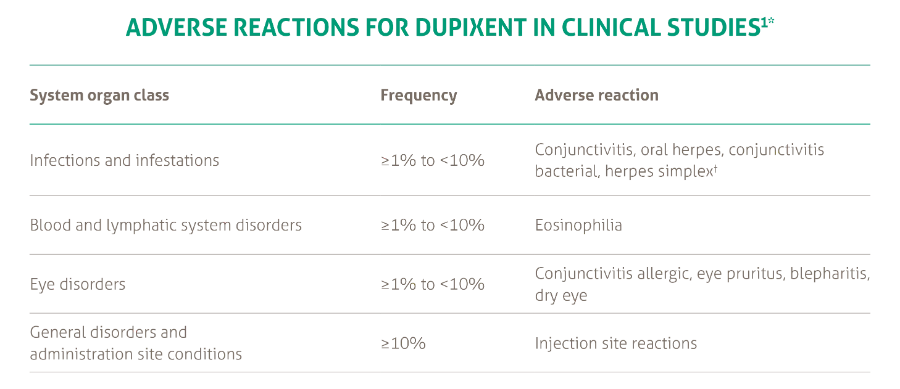
SANA7993_Safety-Page-Tables_V0.2_1_New3
Products_Dermatology_Atopic-Dermatitis_Adverse-Events-Adults_18012021