.png/jcr:content.png)
Measles
Discover timely medical updates and key resources to support the care of those with measles, helping you stay informed and improve patient outcomes.
*Image is not an actual patient.
About measles
The challenges of measles
Measles is one of the most contagious infectious diseases caused by a virus. It is transmitted through infectious droplets and the air when an infected person breathes, sneezes and coughs.
The virus infects the respiratory tract and then spreads throughout the body. Measles occurs exclusively in humans.1 It is characterised by a prodrome of fever and malaise, cough, coryza, and conjunctivitis followed by a maculopapular rash. Measles is often a severe disease with complications including otitis media, pneumonia and diarrhoea.2
No specific antiviral treatment exists for measles virus however, it can be prevented by routine measles vaccination during childhood, combined with mass immunisation campaigns in countries with high case and death rates.1
Supporting measles management through information
Effective management of measles involves a comprehensive understanding of the condition. For healthcare professionals, staying informed about the disease and evolving patient needs is crucial for providing care.
To foster a broader understanding of measles, this page offers a range of selected materials and information.
Understanding measles research and care
Measles is a highly contagious viral disease. Global research aims to better understand, treat, and prevent it, ultimately seeking to eliminate its global presence and improve public health. Broad areas of focus in measles research often include:
- Understanding viral dynamics and immunity
- Advancing prevention strategies, including vaccination
- Improving outbreak response and control measures
- Addressing complications and clinical management
Don’t miss these key links
Signs and symptoms
The first sign of measles is usually a high fever, which begins about 10 to 12 days after exposure to the virus and can be accompanied by a runny nose, cough and red, watery eyes. This prodromal stage lasts around 2-4 days, then a maculopapular rash erupts, usually on the face and upper neck reaching the hands and feet approximately 3 days later. The rash lasts for 5 to 6 days, and then fades.1,2
Common complications from measles include otitis media, pneumonia, and diarrhoea, and are more common and more severe in:2
- Chronically ill patients
- Children under the age of 5yrs
- Adults
Women infected while pregnant are also at risk of severe complications and the pregnancy may end in miscarriage or preterm delivery.1 It is estimated that one to three out of every 1000 children infected with measles will develop severe respiratory and neurologic complications including encephalitis, which can be fatal.3 Severe measles is more likely among poorly nourished young children, especially those with insufficient vitamin A1 or immunocompromised individuals.1
Virology
Measles is caused by a single-stranded, enveloped RNA virus with 1 serotype. It is classified as a member of the genus Morbillivirus in the Paramyxoviridae family. Humans are the only natural hosts of measles virus. The virus is transmitted by direct contact with infectious droplets or by airborne spread when an infected person breathes, coughs, or sneezes. Measles virus can remain infectious in the air for up to two hours after an infected person leaves an area.3
Diagnosis
Measles is usually diagnosed by the presence of clinical symptoms characteristic of the disease, including febrile rash illness especially if the person recently travelled internationally or was exposed to a person with febrile rash illness. Detection of measles-specific IgM antibody and measles RNA by real-time polymerase chain reaction (RT-PCR) from serum sample, throat swab (or nasopharyngeal swab) and urine sample are the most common methods for confirming measles infection.3
Prevention
Measles can be prevented through vaccination. Monovalent measles vaccine is not available in Australia. Measles vaccination is provided using either measles-mumps-rubella (MMR) or measles-mumps-rubella-varicella (MMRV) vaccines.2 Two doses of measles-containing vaccine are recommended for all children ≥ 12 months of age and non-immune adolescents and adults born during or since 1966 especially those working in certain occupations, such as healthcare workers, staff working in early childhood education and care, staff of long-term care facilities and staff of correctional facilities or those travelling internationally. MMRV vaccines are not recommended for use in persons ≥14 years of age.2
MMR-containing vaccines are not routinely recommended for infants <12 months of age.
However, MMR vaccine can be given to children from as early as 6 months of age in certain circumstances, including travel to highly endemic areas and during outbreaks. If the infant is less than 11 months of age, they will still require their routine doses at 12 and 18 months.2 Infected people should be isolated for four days after they develop a rash to prevent spread of the disease to close contacts.3
Close Contacts: Non-immune people who are exposed to measles should receive an MMR vaccine (MMRV in some instances) for post-exposure prophylaxis within 72 hours of exposure. In some settings, normal human immunoglobulin (NHIG), rather than MMR or MMRV, is recommended.2,5
Refer to post-exposure prophylaxis needed within 72 hours of 1st exposure for people exposed to measles.
Epidemiology
Australia was declared measles free by World Health Organization (WHO) in March 2014.2 According to annual immunisation coverage report in 2019, 2-dose vaccine coverage in children aged 5 years was 96.4% in non-indigenous and 98.8% in indigenous children.4
However, measles cases in Australia continue to occur, predominantly in non-immune travelers and their contacts, leading to sporadic measles outbreaks of limited size and duration.2 In 2019, 285 cases of measles were reported in Australia, which was almost three times as many as in 2018.6
The number of measles deaths in Australia has fallen to near zero since vaccination was introduced for all infants. Between 1996 and 2016, only 3 reported deaths were caused by measles.7
Although measles is rare in Australia, evidence suggest an ongoing need to maintain and improve vaccine uptake in vulnerable populations to prevent outbreaks.7
Treatment
No specific antiviral treatment exists for measles virus. Severe complications from measles can be avoided through supportive care that ensures good nutrition, adequate fluid intake and treatment of dehydration with WHO-recommended oral rehydration solution. Antibiotics are recommended to treat eye and ear infections, and pneumonia and vitamin A supplements to prevent eye damage and blindness.1
Featured content

Register to receive full access (Healthcare Professionals Only)
Are you a registered healthcare professional?
Register in less than a minute to access the latest updates and resources to support your practice and help deliver better outcomes for your patients.

Vaccines
We are a leading innovator and one of the world’s largest manufacturers of vaccines. Our company is at the forefront of vaccine development across an expansive and ever-growing range of diseases.
Can’t find what you’re looking for?
Search our extensive knowledge hub
- Measles. World Health Organization Fact Sheet. http://www.who.int/mediacentre/factsheets/fs286/en/. Updated 5 December 2019. Date accessed: November 2021
- Australian Immunisation Handbook 10th edition. Australian Govt. Department of Health. https://immunisationhandbook.health.gov.au/vaccine-preventable-diseases/measles. Date accessed November 2021
- Measles. Centers for Disease Control and Prevention. https://www.cdc.gov/measles/hcp/clinical-overview/?CDC_AAref_Val=https://www.cdc.gov/measles/hcp/index.html Date accessed November 2021
- Annual Immunisation Coverage Report 2019. NCIRS https://ncirs.org.au/annual-immunisation-coverage-report-2022 Date accessed November 2021
- Australian Immunisation Handbook. Table: Post-exposure prophylaxis needed within 72 hours of 1st exposure for people exposed to measles. Available at https://immunisationhandbook.health.gov.au/resources/tables/table-post-exposure-prophylaxis-needed-within-6-days-144-hours-of-1st-exposure-for-people-exposed-to-measles Accessed November 2021
- Measles in Australia. AJGP. https://www1.racgp.org.au/ajgp/2020/march/measles-elimination-in-australia Accessed November 2021
- Measles in Australia. Aust Institute of Health & Welfare. https://www.aihw.gov.au/getmedia/c828baef-75d9-4295-9cc9-b3d50d7153a2/aihw-phe-236_Measles.pdf.aspx Accessed November 2021
Waddling-Gait---Robert,-28-year-old-mild-LOPD-patient
Waddling Gait - Robert, 28-year-old mild LOPD patient
Reaching-Overhead---Robert,-28-year-old-mild-LOPD-patient
Reaching Overhead - Robert, 28-year-old mild LOPD patient
Standing-From-Sitting---Robert,-28-year-old-mild-LOPD-patient
Standing From Sitting - Robert, 28-year-old mild LOPD patient
Climbing-Stairs---Robert,-28-year-old-mild-LOPD-patient
Climbing Stairs - Robert, 28-year-old mild LOPD patient
Waddling-Gait---Karen,-18-year-old-moderate-LOPD-patient

Waddling Gait - Karen, 18-year-old moderate LOPD patient
Reaching-Overhead---Karen,-18-year-old-moderate-LOPD-patient

Reaching Overhead - Karen, 18-year-old moderate LOPD patient
Standing-From-Sitting---Karen,-18-year-old-moderate-LOPD-patient

Standing From Sitting - Karen, 18-year-old moderate LOPD patient
Climbing-Stairs---Karen,-18-year-old-moderate-LOPD-patient

Climbing Stairs - Karen, 18-year-old moderate LOPD patient
ASPIRE-ICT-1-23_Harrington_MAT-AU-2302788-1

ASPIRE-ICT-1-23_Kyle-Blakey_MAT-AU-2302789-1

Which-biologic-and-why--When-to-switch-to-another-one-

Waddling-Gait---Brian,-44-year-old-severe-LOPD-patient

Waddling Gait - Brian, 44-year-old severe LOPD patient
Reaching-Overhead---Brian,-44-year-old-severe-LOPD-patient

Reaching Overhead - Brian, 44-year-old severe LOPD patient
Standing-From-Sitting---Brian,-44-year-old-severe-LOPD-patient

Standing From Sitting - Brian, 44-year-old severe LOPD patient
Climbing-Stairs---Brian,-44-year-old-severe-LOPD-patient

Climbing Stairs - Brian, 44-year-old severe LOPD patient
RESP-ICT2_Wark_MAT-AU-2301970
.webp/jcr:content/RESP-ICT2-Wark_400X300%20(1).webp)
RESP-ICT2_Wark_MAT-AU-2301970
RESP-ICT2_Stone_MAT-AU-2301972
.webp/jcr:content/RESP-ICT2-Stone_400X300%20(1).webp)
RESP-ICT2_Stone_MAT-AU-2301972
Remission-in-rheumatology---Dr-Michelle-Tellus
.webp/jcr:content/RESP-ICT2-Tellus_400X300%20(1).webp)
Remission in rheumatology - Dr Michelle Tellus
Pavord_MAT-AU-2300571

Pavord_MAT-AU-2300571
Wark_MAT-AU-2300572

Wark_MAT-AU-2300572
Q-A-Discussion_MAT-AU-2300573

Q&A-Discussion_MAT-AU-2300573
RESP-ICT3_Tellus_MAT-AU-2302033

RESP-ICT3_Tellus_MAT-AU-2302033
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Hew_MAT-AU-2302035

RESP-ICT3_Hew_MAT-AU-2302035
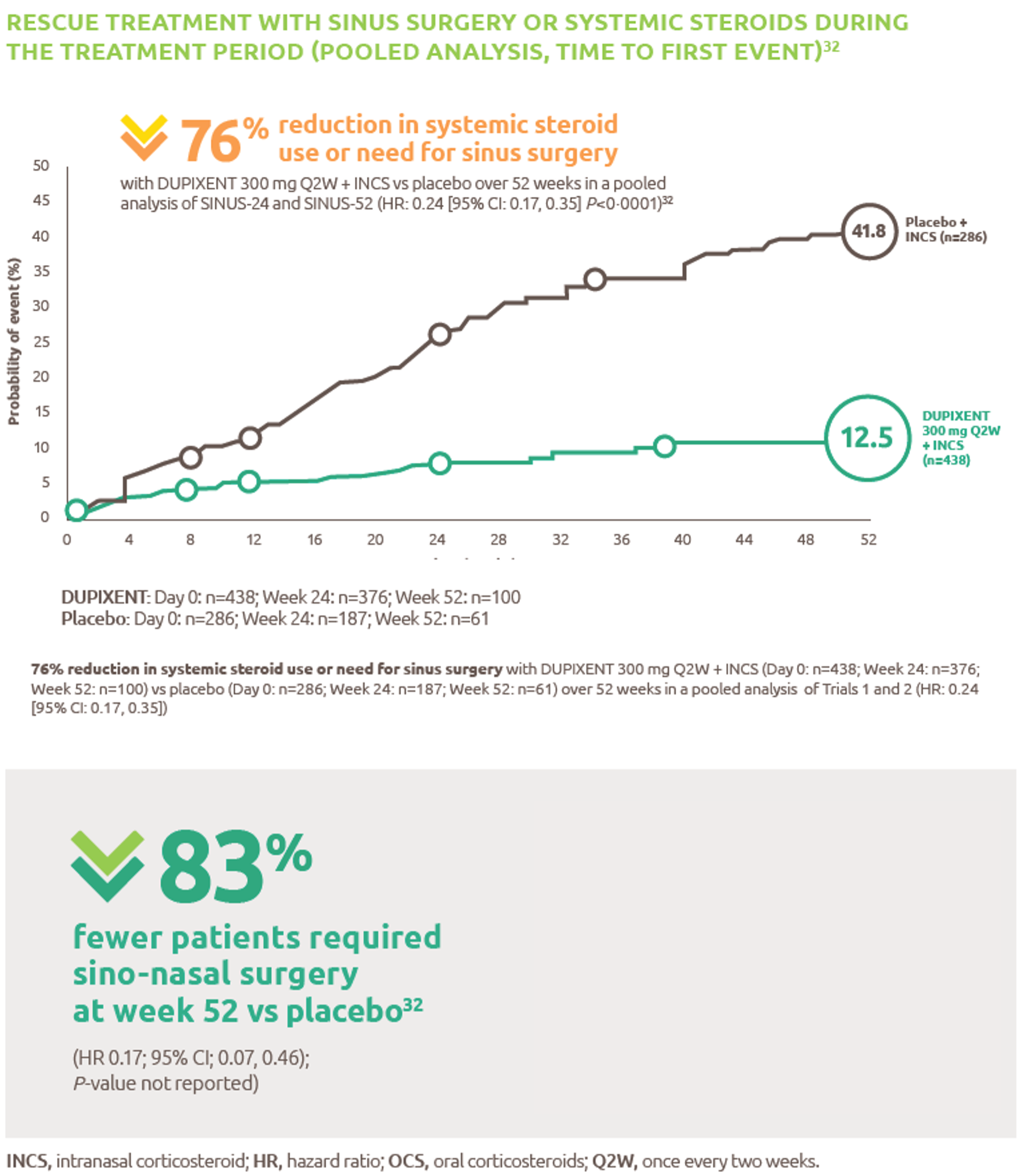
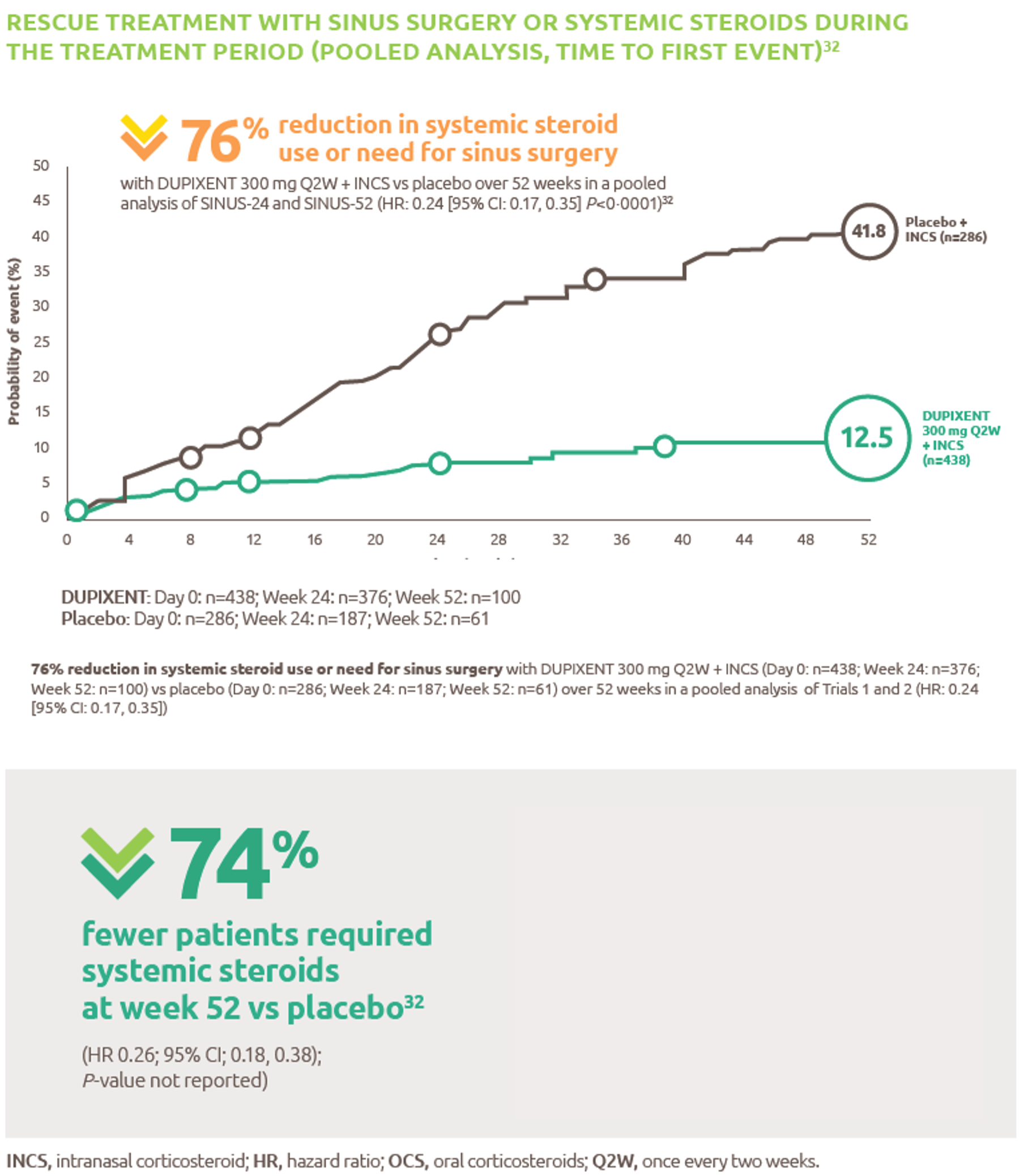
Reduced-need-for-sinus-surgery
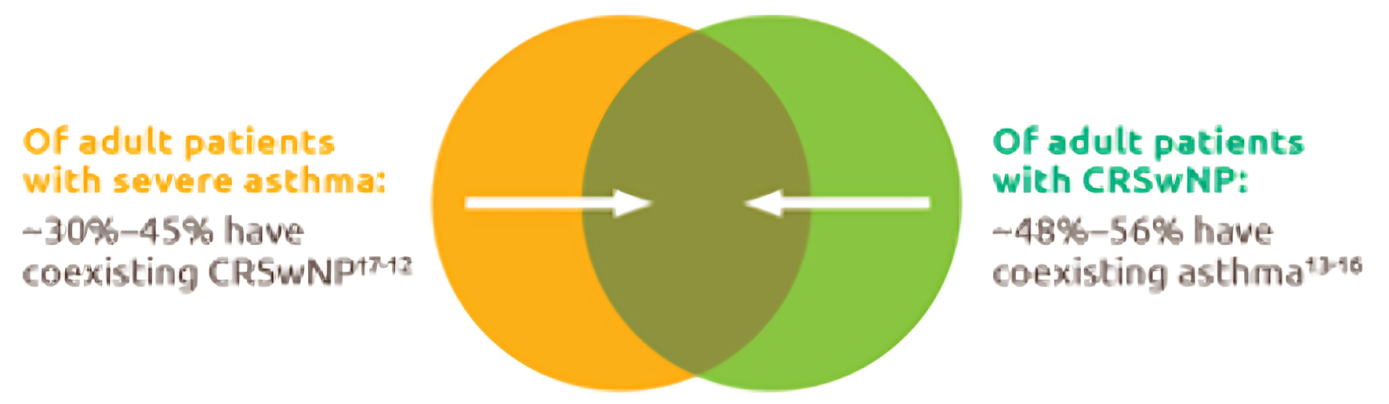
Up-to-45--of-severe-asthma-patients-have-comorbid-CRSwNP
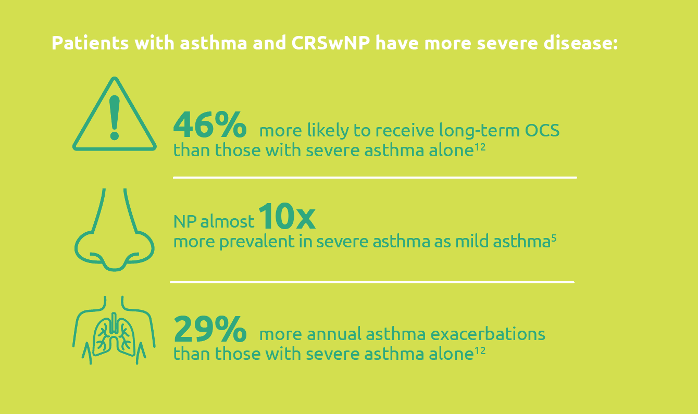
Severe-asthma-with-comorbid-CRSwNP-leads-to-more-severe-disease
.png)
Less-rescue-oral-corticosteriod-use
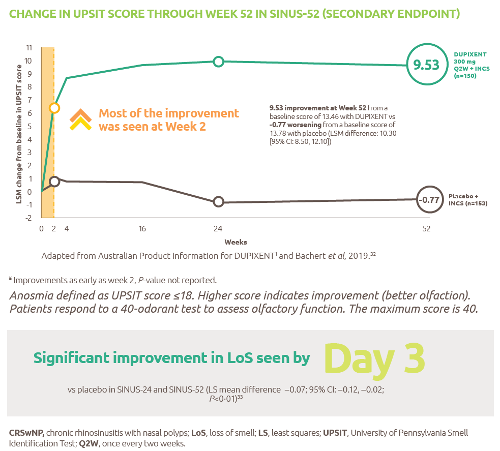
Improved-sense-of-smell
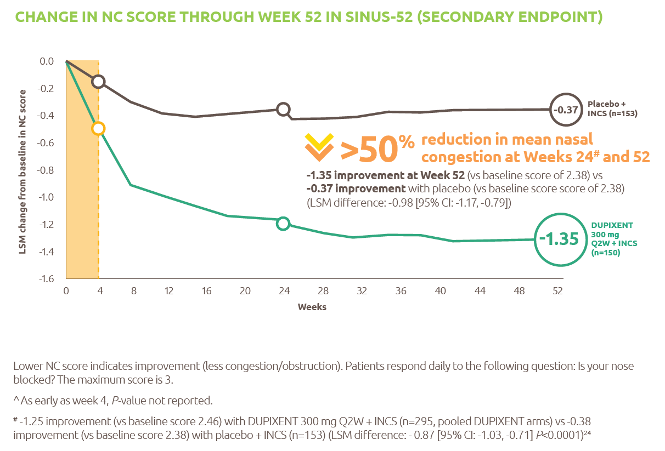
Reduced-obstruction-and-congestion
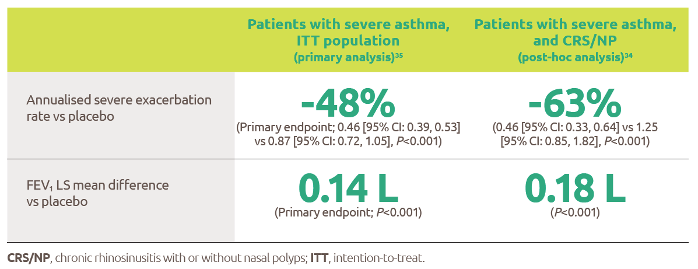
Reduced-asthma-exacerbations-and-improved-lung-function
IL-4-and-IL-13-are-key-and-central-drivers-of-type-2-inflammation

Gaucher-diagnosis-1

RESP-ICT2_Debate_MAT-AU-2301973

RESP-ICT2_Debate_MAT-AU-2301973
RESP-ICT3_Q-A_MAT-AU-2302036

RESP-ICT3_Q&A_MAT-AU-2302036
ASPIRE-ICT1-23_Q-A_MAT-AU-2302791-1

RESP-ICT2_Stone_CS_MAT-AU-2301975

RESP-ICT2_Stone_CS_MAT-AU-2301975
RESP-ICT2_Wark_CS_MAT-AU-2301974

RESP-ICT2_Wark_CS_MAT-AU-2301974
RESP-ICT2_Panel-Discussion_MAT-AU-2301976

RESP-ICT2_Panel-Discussion_MAT-AU-2301976
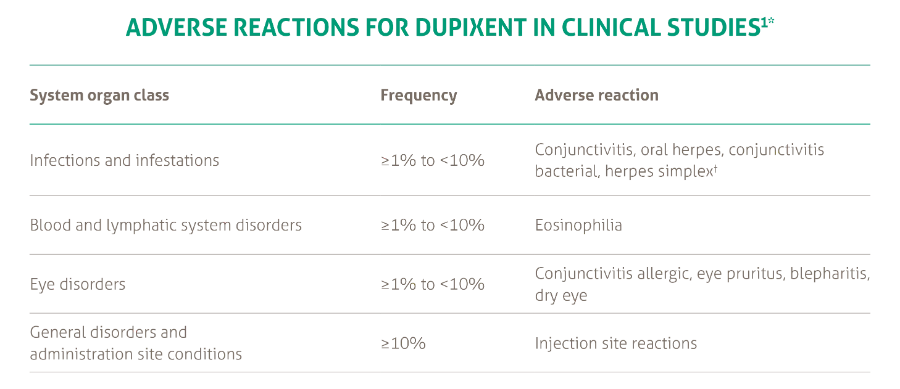
SANA7993_Safety-Page-Tables_V0.2_1_New3
Products_Dermatology_Atopic-Dermatitis_Adverse-Events-Adults_18012021