Typhoid
Discover timely medical updates and key resources on preventing and managing typhoid – helping you stay informed and improve patient outcomes.
*Image is not an actual patient.
About typhoid
The challenges of typhoid
Typhoid fever is a life-threatening infection caused by Salmonella typhi (S.typhi), which is acquired through ingestion of contaminated food or water. It is a febrile disease whose symptoms include fever, headache, nausea, abdominal pain, constipation or diarrhoea and a rash in some cases. Serious complications or death can result from severe cases. The vast majority of S.typhi infections occur in areas with poor sanitation and lack of clean drinking water.1
Supporting typhoid management through information
Effective management of typhoid involves a comprehensive understanding of the condition. For healthcare professionals, staying informed about the disease and evolving patient needs is crucial for providing care.
To foster a broader understanding of typhoid, this page offers a range of selected materials and information.
Understanding typhoid research and care
Effective management and prevention of typhoid begins with equipping healthcare providers with the resources they need to prevent and treat the disease effectively. Here are broad areas of focus for typhoid research:
- Monitoring antibiotic resistance patterns globally to guide treatment protocols
- Administering effective antibiotics based on resistance surveillance
- Rolling out typhoid vaccination programs in endemic regions, alongside water/sanitation improvements
Don’t miss these key links
Signs and symptoms
Typical presenting symptoms of typhoid fever are varied but may include fever, headache, malaise, anorexia, non-productive cough, myalgia, constipation (or diarrhoea in younger patients) and bradycardia. Complications of typhoid fever occur in 10-15% of cases, more commonly in patients who have been ill for more than 2 weeks. Relapse can occur and usually presents 2-3 weeks after the initial fever resolves.2
It has been reported that up to 5% of patients who develop typhoid fever will become chronic carriers, even after treatment. These carriers are an important reservoir in endemic areas, and can be of public health significance in Australia (for example if they worked in the food industry).2
The incubation period for typhoid fever is usually 7-14 days, but can be as early as 3 days and as late as 60 days after infection.2
Diagnosis
The non-specific symptoms associated with typhoid fever make it difficult to distinguish clinically from many other febrile illnesses including dengue fever, malaria and influenza that are also common in typhoid endemic areas.3 Definitive diagnosis of typhoid fever is by positive culture of the organism in the blood, bone marrow, faeces or urine, most commonly isolation of S. typhi from blood.4
Blood culture is preferred over stool or urine cultures. However, a single blood culture is only positive in approximately 50% of cases and multiple cultures may be required as they increase the sensitivity of the test. Bone marrow culture has a higher sensitivity (approximately 80%) and is not commonly affected by previous or concurrent antibiotic use. The sensitivity of stool cultures increases as the duration of the illness increases.5
Prevention
Typhoid is a vaccine preventable disease. However, it is recommended that travellers also be advised about personal hygiene, food safety and drinking boiled or bottled water only. They should be advised that raw (or undercooked) shellfish, salads, cold meats, untreated water and ice (in drinks) are all potentially ‘high-risk’, as are short (day) trips away from higher quality accommodation venues.2
Bacteriology
Typhoid fever is caused by the bacterium Salmonella enterica subspecies enterica serovar Typhi (commonly referred to as S. typhi). Paratyphoid fever, caused by infection with S. enterica serovar Paratyphi A or B, is clinically indistinguishable from typhoid fever. The two infections are endemic in similar geographic areas.2 Humans are the sole reservoir of S. typhi and transmission occurs via ingesting faecally contaminated food and water.2
Epidemiology
The vast majority of typhoid fever cases occur in less developed countries, where poor sanitation, poor food hygiene and untreated drinking water all contribute to endemic disease, with moderate to high incidence. Regions with a high incidence of typhoid fever (>100 cases per 100,000 population per year) include the Indian subcontinent, most Southeast Asian countries and several South Pacific nations, including Papua New Guinea.2
In developed countries including Australia, typhoid fever is predominantly a travel related disease, with a considerably greater risk following travel to the Indian subcontinent than to other regions.2 Those who travel to endemic regions to visit friends and relatives (e.g. immigrants who travel to their former homelands) appear to be at considerably greater risk of acquiring typhoid fever than other travellers.2
There are typically fewer than 150 cases of typhoid fever reported in Australia each year and most occur following travel to regions with endemic disease.2
Treatment
Without therapy, the illness can last for 3 to 4 weeks and death rates range between 12 – 30%.6 Antibiotic treatment shortens the duration of typhoid fever and reduces the risk of death.5 In the pre-antibiotic era, typhoid fever was associated with a fatality rate of between 10 and 20%, however with antibiotic treatment this was reduced to 1-4%.3
Resistance to antibiotics is increasing, with resistance to chloramphenicol being observed in the early 1970’s, and more recently reduced susceptibility to fluoroquinolones and cephalosporins has emerged. Sporadic resistance to azithromycin has also been reported.1,3
The first case of an extensively drug-resistant (XDR) strain of S. typhi has been reported in Australia in a 20-month-old traveler returning from Pakistan. The blood and stool cultures grew a strain with resistance to chloramphenicol, ampicillin, trimethoprim– sulfamethoxazole, fluoroquinolones and third-generation cephalosporins. The patient was successfully treated with meropenem and azithromycin.7
A chronic carrier state, in which stool or urine cultures for Salmonella typhi remain positive for more than one year, occurs in up to 5% of infected people.6
Featured content

Register to receive full access (Healthcare Professionals Only)
Are you a registered healthcare professional?
Register in less than a minute to access the latest updates and resources to support your practice and help deliver better outcomes for your patients.
Can’t find what you’re looking for?
Search our extensive Content Library
- World Health Organisation. Typhoid. www.who.int/health-topics/typhoid#tab=tab_1 (Accessed August 2024)
- Australian Immunisation Handbook. https://immunisationhandbook.health.gov.au/contents/vaccine-preventable-diseases/typhoid-fever (Accessed August 2024)
- World Health Organisation. SAGE Background Paper on Typhoid Vaccines for SAGE Meeting (October 2017). https://cdn.who.int/media/docs/default-source/immunization/position_paper_documents/typhoid/1-typhoid-sage-background-paper-final-v3b.pdf?sfvrsn=ddf418c3_2 Accessed August 2024
- NSW Health. Typhoid and paratyphoid fevers control guideline. https://www.health.nsw.gov.au/Infectious/controlguideline/Pages/typhoid.aspx Last updated July 2019. Accessed August 2024.
- CDC Yellow Book. Chapter 4. Typhoid and paratyphoid fever. https://wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/typhoid-and-paratyphoid-fever Accessed August 2024
- Centres for Disease Control & Prevention. Typhoid https://www.cdc.gov/typhoid-fever/hcp/clinical-guidance/index.html#:~:text=About%201%25%E2%80%934%25%20of%20people%20with%20typhoid%20fever%20become,for%20Salmonella%20Typhi%20for%20more%20than%20one%20year. (Accessed August 2024)
- Howard-Jones, A et.al. First reported case of extensively drug-resistant typhoid in Australia. https://onlinelibrary.wiley.com/doi/full/10.5694/mja2.50316 MJA
MAT-AU-2101888 - 2.0 - 08/2024
Waddling-Gait---Robert,-28-year-old-mild-LOPD-patient
Waddling Gait - Robert, 28-year-old mild LOPD patient
Reaching-Overhead---Robert,-28-year-old-mild-LOPD-patient
Reaching Overhead - Robert, 28-year-old mild LOPD patient
Standing-From-Sitting---Robert,-28-year-old-mild-LOPD-patient
Standing From Sitting - Robert, 28-year-old mild LOPD patient
Climbing-Stairs---Robert,-28-year-old-mild-LOPD-patient
Climbing Stairs - Robert, 28-year-old mild LOPD patient
Waddling-Gait---Karen,-18-year-old-moderate-LOPD-patient

Waddling Gait - Karen, 18-year-old moderate LOPD patient
Reaching-Overhead---Karen,-18-year-old-moderate-LOPD-patient

Reaching Overhead - Karen, 18-year-old moderate LOPD patient
Standing-From-Sitting---Karen,-18-year-old-moderate-LOPD-patient

Standing From Sitting - Karen, 18-year-old moderate LOPD patient
Climbing-Stairs---Karen,-18-year-old-moderate-LOPD-patient

Climbing Stairs - Karen, 18-year-old moderate LOPD patient
ASPIRE-ICT-1-23_Harrington_MAT-AU-2302788-1

ASPIRE-ICT-1-23_Kyle-Blakey_MAT-AU-2302789-1

Which-biologic-and-why--When-to-switch-to-another-one-

Waddling-Gait---Brian,-44-year-old-severe-LOPD-patient

Waddling Gait - Brian, 44-year-old severe LOPD patient
Reaching-Overhead---Brian,-44-year-old-severe-LOPD-patient

Reaching Overhead - Brian, 44-year-old severe LOPD patient
Standing-From-Sitting---Brian,-44-year-old-severe-LOPD-patient

Standing From Sitting - Brian, 44-year-old severe LOPD patient
Climbing-Stairs---Brian,-44-year-old-severe-LOPD-patient

Climbing Stairs - Brian, 44-year-old severe LOPD patient
RESP-ICT2_Wark_MAT-AU-2301970
.webp/jcr:content/RESP-ICT2-Wark_400X300%20(1).webp)
RESP-ICT2_Wark_MAT-AU-2301970
RESP-ICT2_Stone_MAT-AU-2301972
.webp/jcr:content/RESP-ICT2-Stone_400X300%20(1).webp)
RESP-ICT2_Stone_MAT-AU-2301972
Remission-in-rheumatology---Dr-Michelle-Tellus
.webp/jcr:content/RESP-ICT2-Tellus_400X300%20(1).webp)
Remission in rheumatology - Dr Michelle Tellus
Pavord_MAT-AU-2300571

Pavord_MAT-AU-2300571
Wark_MAT-AU-2300572

Wark_MAT-AU-2300572
Q-A-Discussion_MAT-AU-2300573

Q&A-Discussion_MAT-AU-2300573
RESP-ICT3_Tellus_MAT-AU-2302033

RESP-ICT3_Tellus_MAT-AU-2302033
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Hew_MAT-AU-2302035

RESP-ICT3_Hew_MAT-AU-2302035
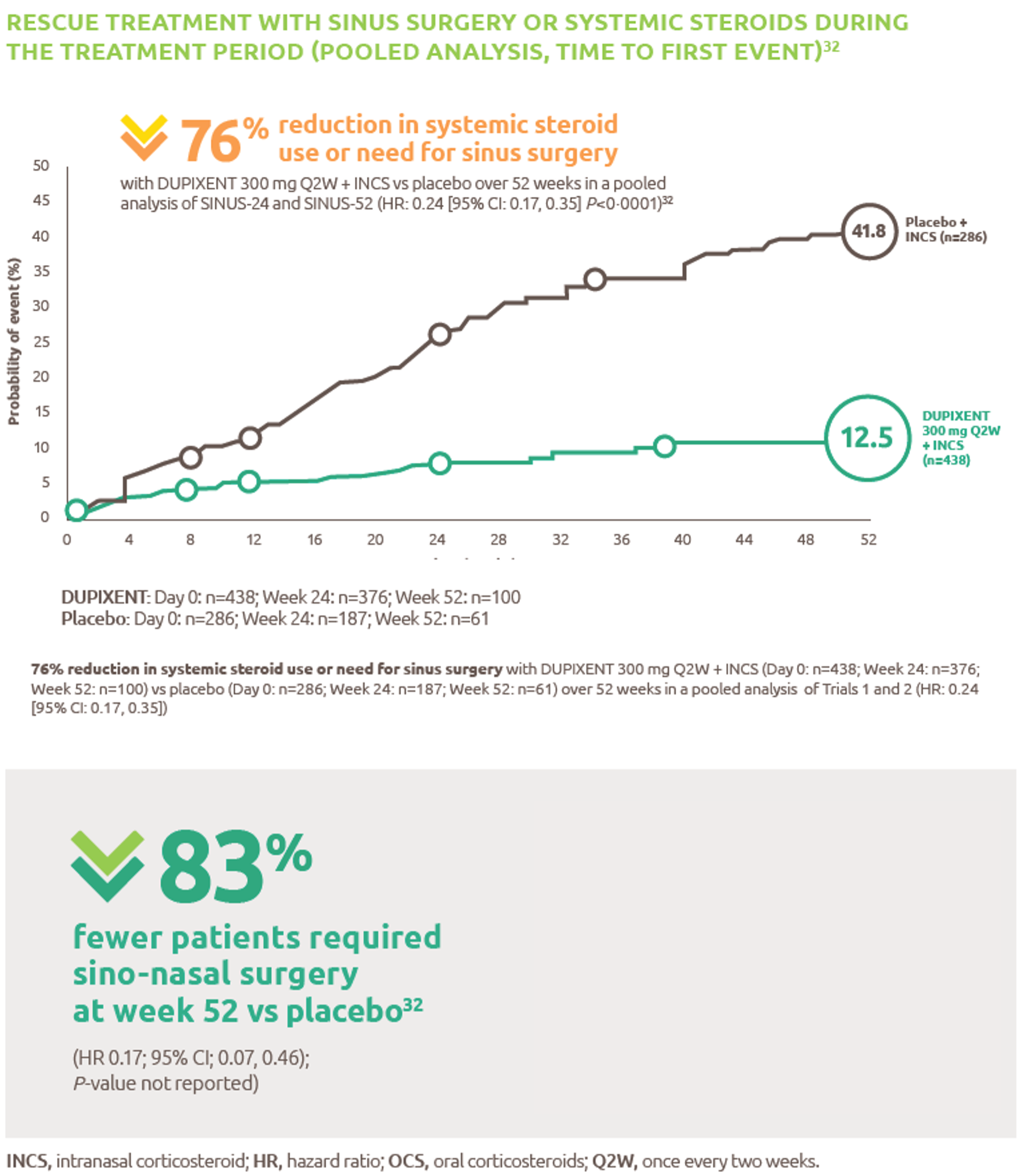
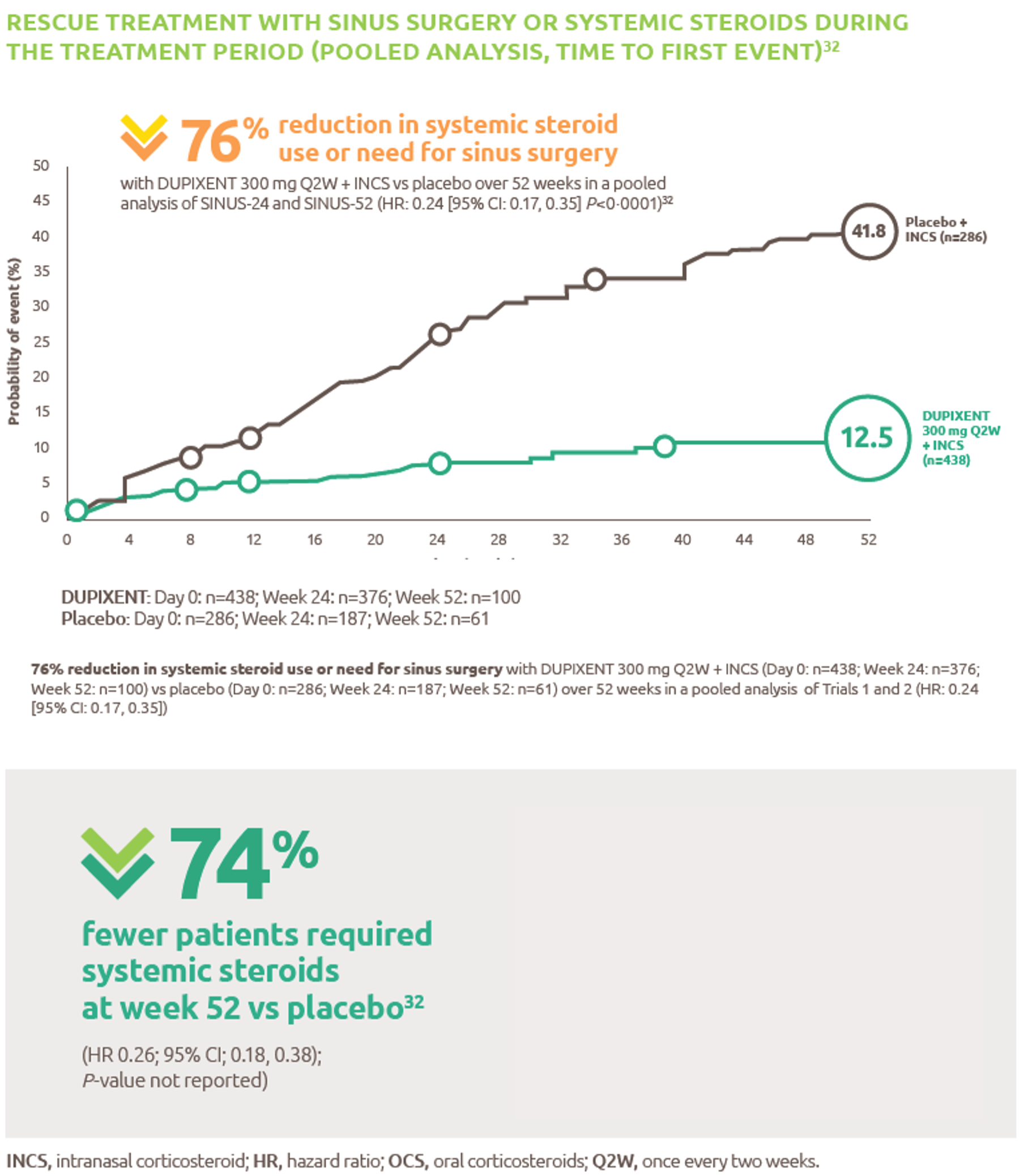
Reduced-need-for-sinus-surgery
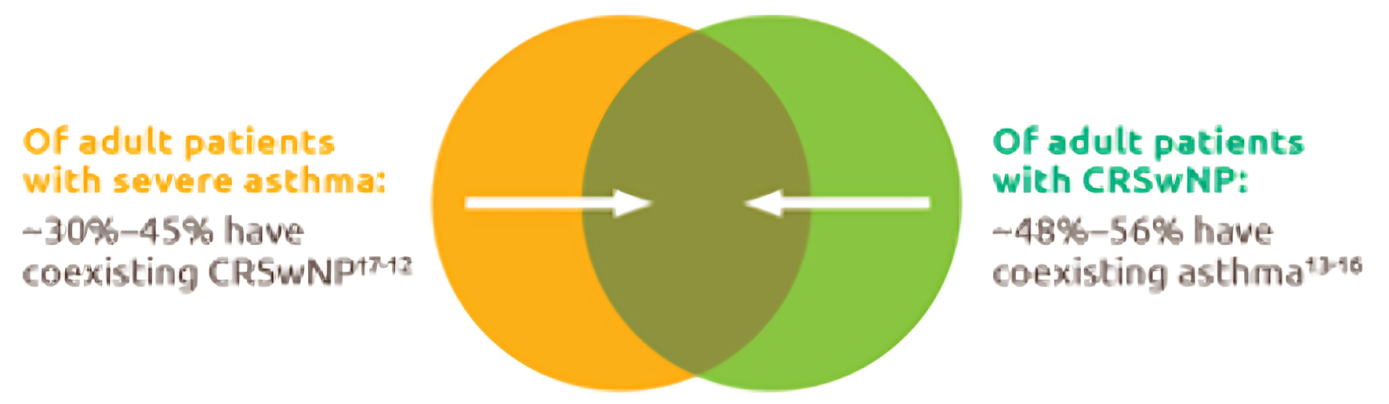
Up-to-45--of-severe-asthma-patients-have-comorbid-CRSwNP
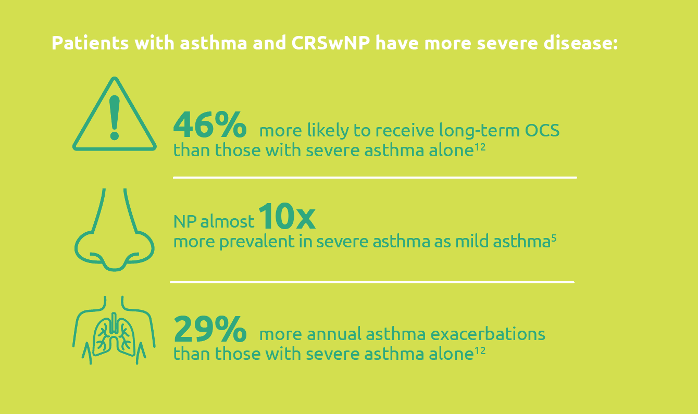
Severe-asthma-with-comorbid-CRSwNP-leads-to-more-severe-disease
.png)
Less-rescue-oral-corticosteriod-use
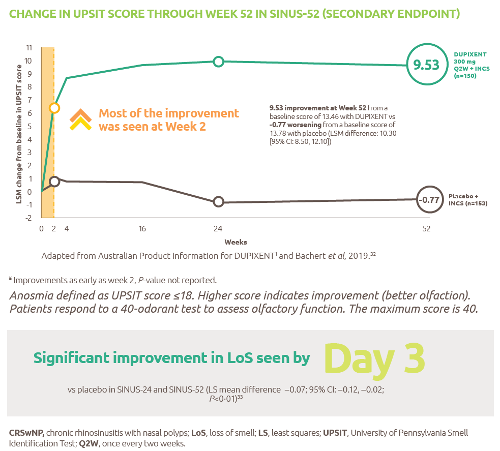
Improved-sense-of-smell
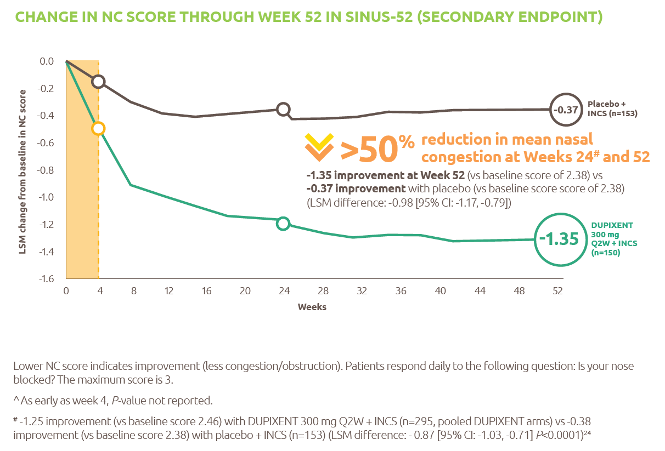
Reduced-obstruction-and-congestion
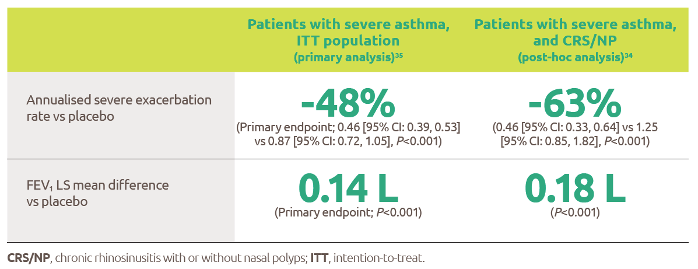
Reduced-asthma-exacerbations-and-improved-lung-function
IL-4-and-IL-13-are-key-and-central-drivers-of-type-2-inflammation

Gaucher-diagnosis-1

RESP-ICT2_Debate_MAT-AU-2301973

RESP-ICT2_Debate_MAT-AU-2301973
RESP-ICT3_Q-A_MAT-AU-2302036

RESP-ICT3_Q&A_MAT-AU-2302036
ASPIRE-ICT1-23_Q-A_MAT-AU-2302791-1

RESP-ICT2_Stone_CS_MAT-AU-2301975

RESP-ICT2_Stone_CS_MAT-AU-2301975
RESP-ICT2_Wark_CS_MAT-AU-2301974

RESP-ICT2_Wark_CS_MAT-AU-2301974
RESP-ICT2_Panel-Discussion_MAT-AU-2301976

RESP-ICT2_Panel-Discussion_MAT-AU-2301976
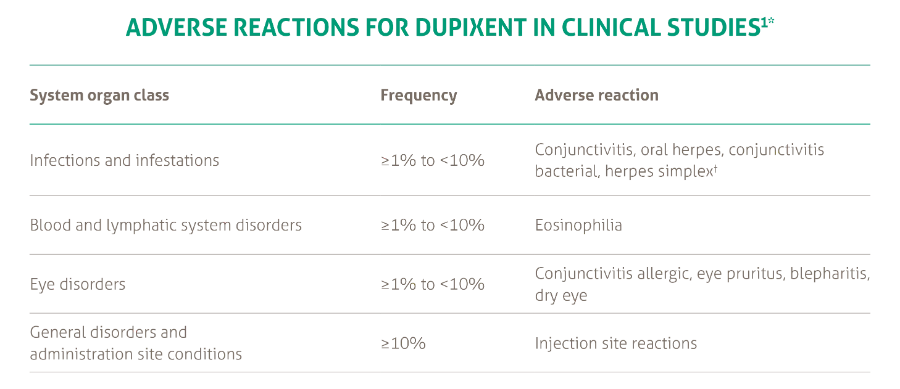
SANA7993_Safety-Page-Tables_V0.2_1_New3
Products_Dermatology_Atopic-Dermatitis_Adverse-Events-Adults_18012021