.png/jcr:content.png)
Hepatitis A
Discover timely medical updates and key resources on prevention and control of hepatitis A - helping you stay informed and improve patient outcomes
*Image is not an actual patient.
About hepatitis A
The challenges of hepatitis A
Hepatitis A is a viral infection of the liver. It most commonly presents as a mild illness which resolves within one to two months, but can be a more severe illness persisting for several months.1,2 The hepatitis A virus (HAV) is transmitted through ingestion of food and water that is contaminated with the faeces of an infected person or through direct contact with an infectious person. The risk of hepatitis A infection is associated with a lack of clean water, and poor sanitation and hygiene (such as poor handwashing).2
There is no specific treatment for the disease and the best way to prevent hepatitis A is through improved hygiene, sanitation and vaccination with the hepatitis A vaccine.2
Supporting hepatitis A through information
Effective management and prevention of hepatitis A involves a comprehensive understanding of the condition. For healthcare professionals, staying informed about the disease and evolving epidemiology and science is crucial for providing care.
To foster a broader understanding of hepatitis A, this page offers a range of selected materials and information.
Understanding hepatitis A research and care
Hepatitis A is a contagious liver infection caused by the hepatitis A virus (HAV). Global research aims to better understand, treat, and prevent it, ultimately seeking to control its transmission and improve public health. Broad areas of focus in Hepatitis A research often include:
- Understanding viral epidemiology and transmission
- Advancing prevention strategies, including vaccination
- Improving outbreak response and control
- Addressing public health interventions and hygiene
Don’t miss these key links
Signs and symptoms
The incubation period for hepatitis A is usually 14–28 days.2 It is a highly contagious illness and infected people can excrete the virus in their faeces up to 2 weeks before the onset of symptoms and at least one week after the illness.3
Symptoms of hepatitis A can include fever, malaise, loss of appetite, diarrhoea, nausea, abdominal discomfort, dark-coloured urine, jaundice, vomiting, clay-coloured bowel movements, fatigue and joint pain. Not everyone who is infected will have all of the symptoms.3 Symptoms usually last less than 2 months, although some people can have relapsing disease for as long as 6 months.1
Adults will show symptoms of illness more often than children, and hepatitis A tends to be more severe in older age groups. Jaundice will occur in more than 70% of older children and adults. In comparison, infected children under 6 years of age do not usually experience noticeable symptoms, and only 10% will develop jaundice.2 Complications related to hepatitis A infection are uncommon and only rarely will it develop into fulminant hepatitis. Hepatitis A does not cause chronic liver disease. Relapse can occur in about 10% of cases, however it is followed by recovery. Infection with hepatitis A provides lifetime immunity.3
Virology
Hepatitis A is caused by the hepatitis A virus (HAV), a picornavirus (a small single-stranded RNA virus).3 The virus can survive outside the human host in the environment for prolonged periods. It persists on hands for several hours and in food kept at room temperature for considerably longer. Hepatitis A virus is relatively resistant to heat and freezing does not inactivate the virus.3
Diagnosis
Cases of hepatitis A are not clinically distinguishable from other types of acute viral hepatitis. Diagnosis is confirmed by detection of HAV-specific Immunoglobulin G (IgM) antibodies in the blood. Additional tests include reverse transcriptase polymerase chain reaction (RT-PCR) may also be used to detect the hepatitis A virus RNA.2
Prevention
The most effective ways to prevent hepatitis A include improved sanitation and hygiene, food safety and immunisation.2
Hepatitis A vaccination is recommended for persons with an increased risk of acquiring hepatitis A and/or who are at increased risk of severe disease including:3
- Aboriginal and Torres Strait Islander children residing in the Northern Territory, Queensland, South Australia and Western Australia.
- Travellers (≥1 year of age) to moderately to highly endemic areas for hepatitis A.
- Persons whose occupation puts them at increased risk of acquiring hepatitis A such as persons who live or work in rural and remote Indigenous communities and/or persons who regularly provide care for Aboriginal and Torres Strait Islander children in the Northern Territory, Queensland, South Australia and Western Australia; staff working in early childhood education and care; carers of persons with developmental disabilities; and plumbers or sewage workers.
- Persons whose lifestyle puts them at increased risk of acquiring hepatitis A such as those who engage in certain sexual practices (including men who have sex with men and sex industry workers), persons who inject drugs and inmates of correctional facilities.
- Persons with developmental disabilities.
- Persons with chronic liver disease, liver solid organ transplant recipients and/or those chronically infected with either hepatitis B or hepatitis C viruses.
Epidemiology
While hepatitis A was a considerable public health problem in Australia in the 1990’s, local outbreaks of hepatitis A have been decreasing in recent years. It is now an infection more related to travel to countries where hepatitis A is still endemic. Areas of high endemicity include parts of Africa, Asia, Central America and South America.3
Australia has had a hepatitis A vaccination program running for Aboriginal and Torres Strait Islanders since 1999. The program originally commenced in Queensland and was extended to include the Northern Territory, South Australia and Western Australia in 2005. This program has substantially reduced the number of notifications and hospitalisations for hepatitis A in this population. However this group remains at an increased risk of hepatitis A compared with non-Indigenous populations and the vaccination program is ongoing.3
Treatment
There is no specific treatment for hepatitis A. Hospitalisation is usually unnecessary, but recovery from symptoms following infection may be slow and may take several weeks or months. Avoiding unnecessary medications is important. Acetamiophen, paracetamol and medications against vomiting should be avoided. Rest, good nutrition and replacement of fluids lost from vomiting and diarrhoea is recommended.2
Contacts of an infectious person may require post-exposure prophylaxis using hepatitis A vaccine or immunoglobulin. Refer to the most recent version of the Hepatitis A National Guidelines for Public Health Units for further information.3
Featured content

Register to receive full access (Healthcare Professionals Only)
Are you a registered healthcare professional?
Register in less than a minute to access the latest updates and resources to support your practice and help deliver better outcomes for your patients.
Can’t find what you’re looking for?
Search our extensive Content Library
- Hepatitis A Questions and Answers for the Public. Centers for Disease Control and Prevention. What is Hepatitis A - FAQ | CDC July 2020. Accessed April 2022
- Hepatitis A. World Health Organization Fact sheet. http://www.who.int/mediacentre/factsheets/fs328/en/. Reviewed July 2021. Accessed April 2022
- Australian Immunisation Handbook 10th edition. Australian Govt. Department of health. https://immunisationhandbook.health.gov.au/vaccine-preventable-diseases/hepatitis-a Accessed April 2022
MAT-AU-2201306 - 2.0 - 06/2024
Waddling-Gait---Robert,-28-year-old-mild-LOPD-patient
Waddling Gait - Robert, 28-year-old mild LOPD patient
Reaching-Overhead---Robert,-28-year-old-mild-LOPD-patient
Reaching Overhead - Robert, 28-year-old mild LOPD patient
Standing-From-Sitting---Robert,-28-year-old-mild-LOPD-patient
Standing From Sitting - Robert, 28-year-old mild LOPD patient
Climbing-Stairs---Robert,-28-year-old-mild-LOPD-patient
Climbing Stairs - Robert, 28-year-old mild LOPD patient
Waddling-Gait---Karen,-18-year-old-moderate-LOPD-patient

Waddling Gait - Karen, 18-year-old moderate LOPD patient
Reaching-Overhead---Karen,-18-year-old-moderate-LOPD-patient

Reaching Overhead - Karen, 18-year-old moderate LOPD patient
Standing-From-Sitting---Karen,-18-year-old-moderate-LOPD-patient

Standing From Sitting - Karen, 18-year-old moderate LOPD patient
Climbing-Stairs---Karen,-18-year-old-moderate-LOPD-patient

Climbing Stairs - Karen, 18-year-old moderate LOPD patient
ASPIRE-ICT-1-23_Harrington_MAT-AU-2302788-1

ASPIRE-ICT-1-23_Kyle-Blakey_MAT-AU-2302789-1

Which-biologic-and-why--When-to-switch-to-another-one-

Waddling-Gait---Brian,-44-year-old-severe-LOPD-patient

Waddling Gait - Brian, 44-year-old severe LOPD patient
Reaching-Overhead---Brian,-44-year-old-severe-LOPD-patient

Reaching Overhead - Brian, 44-year-old severe LOPD patient
Standing-From-Sitting---Brian,-44-year-old-severe-LOPD-patient

Standing From Sitting - Brian, 44-year-old severe LOPD patient
Climbing-Stairs---Brian,-44-year-old-severe-LOPD-patient

Climbing Stairs - Brian, 44-year-old severe LOPD patient
RESP-ICT2_Wark_MAT-AU-2301970
.webp/jcr:content/RESP-ICT2-Wark_400X300%20(1).webp)
RESP-ICT2_Wark_MAT-AU-2301970
RESP-ICT2_Stone_MAT-AU-2301972
.webp/jcr:content/RESP-ICT2-Stone_400X300%20(1).webp)
RESP-ICT2_Stone_MAT-AU-2301972
Remission-in-rheumatology---Dr-Michelle-Tellus
.webp/jcr:content/RESP-ICT2-Tellus_400X300%20(1).webp)
Remission in rheumatology - Dr Michelle Tellus
Pavord_MAT-AU-2300571

Pavord_MAT-AU-2300571
Wark_MAT-AU-2300572

Wark_MAT-AU-2300572
Q-A-Discussion_MAT-AU-2300573

Q&A-Discussion_MAT-AU-2300573
RESP-ICT3_Tellus_MAT-AU-2302033

RESP-ICT3_Tellus_MAT-AU-2302033
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Hew_MAT-AU-2302035

RESP-ICT3_Hew_MAT-AU-2302035
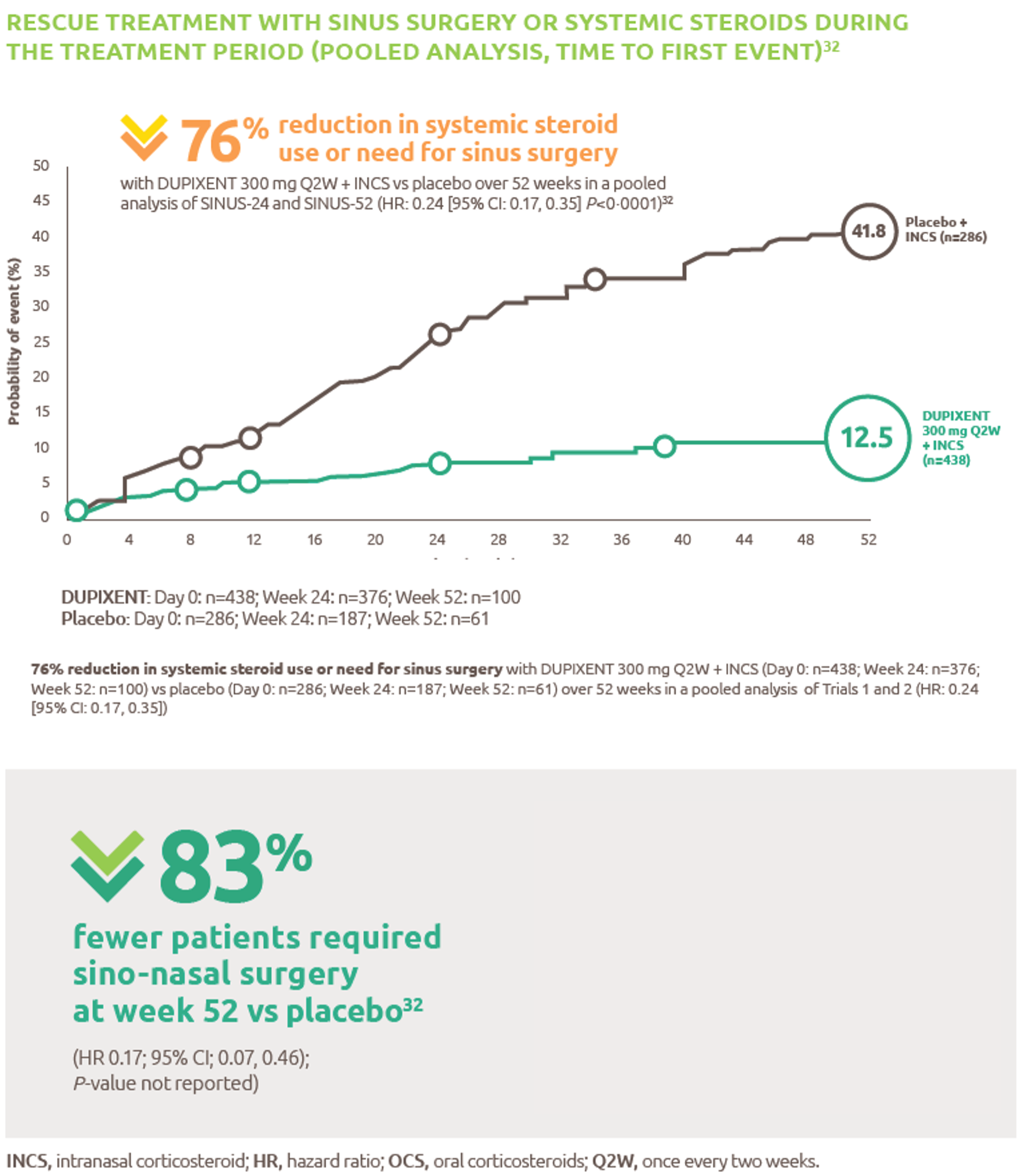
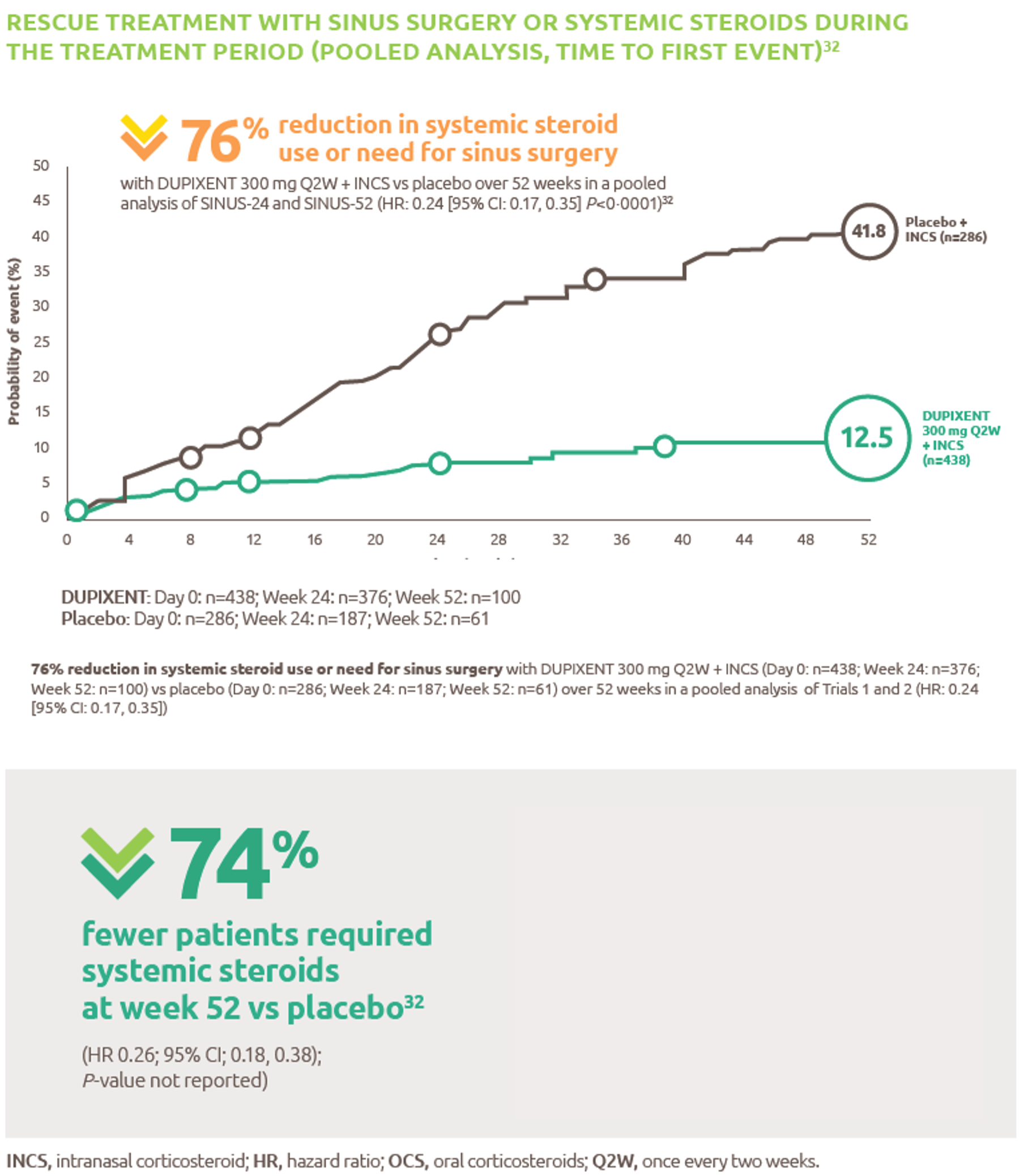
Reduced-need-for-sinus-surgery
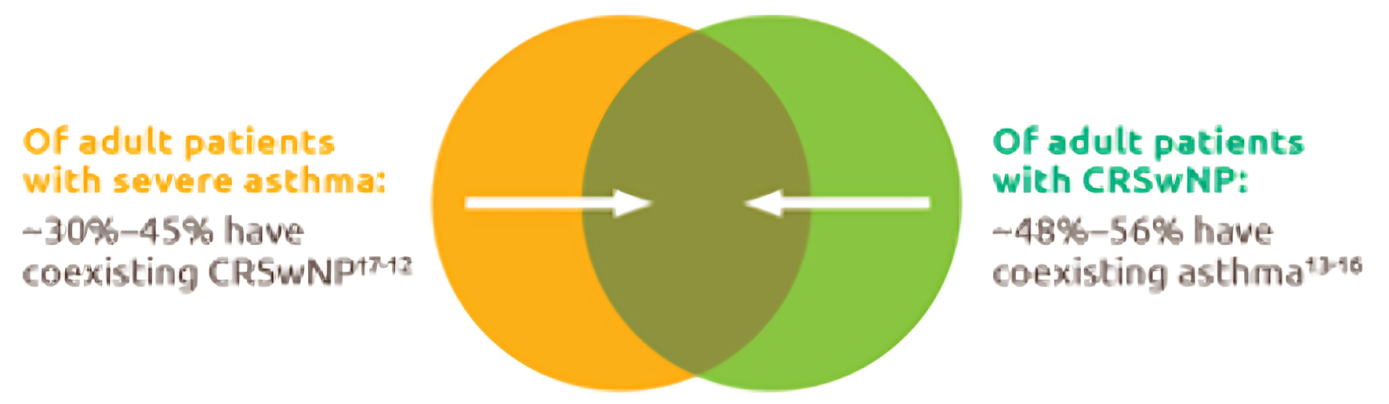
Up-to-45--of-severe-asthma-patients-have-comorbid-CRSwNP
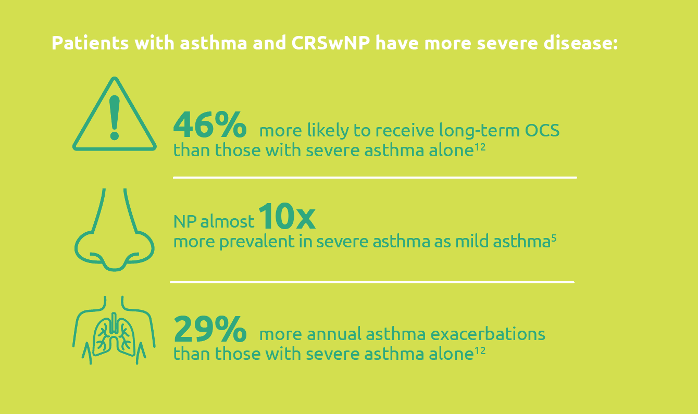
Severe-asthma-with-comorbid-CRSwNP-leads-to-more-severe-disease
.png)
Less-rescue-oral-corticosteriod-use
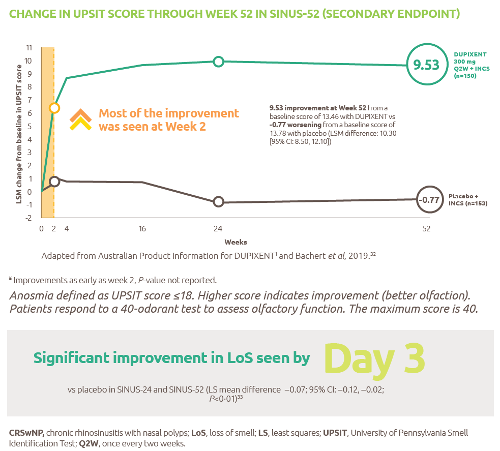
Improved-sense-of-smell
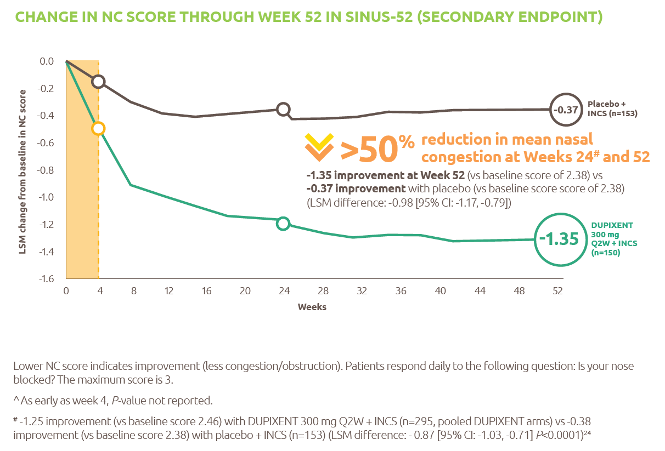
Reduced-obstruction-and-congestion
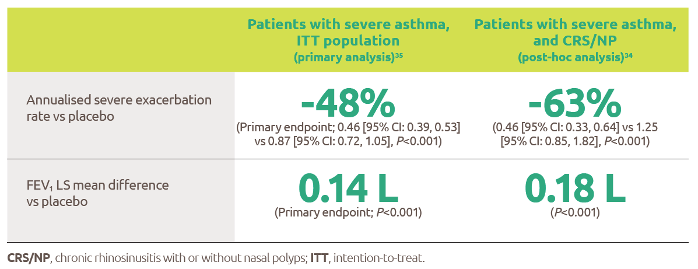
Reduced-asthma-exacerbations-and-improved-lung-function
IL-4-and-IL-13-are-key-and-central-drivers-of-type-2-inflammation

Gaucher-diagnosis-1

RESP-ICT2_Debate_MAT-AU-2301973

RESP-ICT2_Debate_MAT-AU-2301973
RESP-ICT3_Q-A_MAT-AU-2302036

RESP-ICT3_Q&A_MAT-AU-2302036
ASPIRE-ICT1-23_Q-A_MAT-AU-2302791-1

RESP-ICT2_Stone_CS_MAT-AU-2301975

RESP-ICT2_Stone_CS_MAT-AU-2301975
RESP-ICT2_Wark_CS_MAT-AU-2301974

RESP-ICT2_Wark_CS_MAT-AU-2301974
RESP-ICT2_Panel-Discussion_MAT-AU-2301976

RESP-ICT2_Panel-Discussion_MAT-AU-2301976
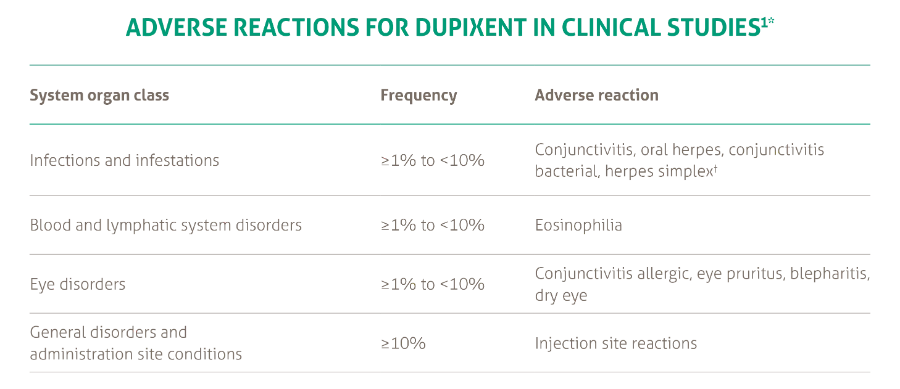
SANA7993_Safety-Page-Tables_V0.2_1_New3
Products_Dermatology_Atopic-Dermatitis_Adverse-Events-Adults_18012021