Japanese encephalitis
Discover timely medical updates and key resources on preventing and controlling japanese encephalitis – helping you stay informed and improve patient outcomes.
*Image is not an actual patient.
About Japanese encephalitis
The challenges of Japanese encephalitis
Japanese encephalitis virus is transmitted to humans through the bites of infected Culex species mosquitoes, particularly Culex tritaeniorhynchus. Japanese encephalitis virus is the leading cause of vaccine-preventable encephalitis in Asia and the western Pacific. For most travelers to Asia, the risk for Japanese encephalitis is very low but varies based on destination, length of travel, season, and activities.
Supporting Japanese encephalitis management through information
Effective management and prevention of Japanese encephalitis involves a comprehensive understanding of the condition. For healthcare professionals, staying informed about the disease and evolving epidemiology and science is crucial for providing care.
To foster a broader understanding of Japanese encephalitis, this page offers a range of selected materials and information
Understanding Japanese encephalitis research and care
Japanese encephalitis (JE) is a severe mosquito-borne viral brain infection. Global research aims to better understand, treat, and prevent it, ultimately seeking to control its spread and improve patient outcomes. Broad areas of focus in Japanese encephalitis research often include:
- Understanding vector-borne transmission and ecology
- Advancing prevention strategies, including vaccination
- Improving diagnosis and clinical management
- Addressing neurological sequelae and long-term care
Don’t miss these key links
Signs and symptoms
The incubation period for JE is 5-15 days.1 While symptomatic disease is rare, in those persons who develop symptoms these usually commence with fever, headache and vomiting.1 Over the next few days mental status changes, weakness, movement disorders and other neurologic symptoms develop.1 JE is a significant public health problem in many parts of Asia, and occasional outbreaks have occurred in Torres Strait. JE has a high case-fatality rate of around 30%. Around 50% of people who survive the acute illness will have neurological sequelae.2
Virology
Japanese encephalitis (JE) is caused by infection with the mosquito-borne JE virus. The disease mainly affects the central nervous system.2
Diagnosis
Individuals who live in or have travelled to a JE-endemic area and experience encephalitis are considered a suspected JE case. To confirm JE virus infection and to investigate other causes of encephalitis requires a laboratory testing of serum or, preferentially, cerebrospinal fluid (CSF).1
Clinical laboratory findings might include a moderate leucocytosis, mild anaemia, and hyponatremia. CSF typically has a mild to moderate pleocytosis with a lymphocytic predominance, slightly elevated protein, and normal ratio of CSF to plasma glucose. Magnetic resonance imaging (MRI) of the brain is better than computed tomography (CT) for detecting JE virus-associated abnormalities. Thalamic lesions are the most commonly described abnormality; which can be highly specific for JE but not a very sensitive marker. EEG abnormalities may include theta and delta coma, burst suppression, epileptiform activity, and occasionally alpha coma.1
Prevention
All travellers to Japanese encephalitis-endemic areas should take precautions to avoid mosquito bites to reduce the risk for JE and other mosquito-borne infectious diseases. Personal preventive measures include the use of repellents (such as those containing DEET, IR3535, picaridin or oil of lemon eucalyptus), long-sleeved clothes, sleeping in screened areas or under mosquito nets.1
Vaccinations are also available in Australia for prevention of Japanese encephalitis.
Epidemiology
Japanese encephalitis (JE) has been a significant public health problem in many parts of Asia, including the Indian subcontinent, Southeast Asia and China and in recent decades it has extended to eastern Indonesia (including Bali) and Papua New Guinea.2
Occasional outbreaks were reported in the Torres Strait from 1995-1998, No cases have been reported in the Torres Strait since 1998; most communities have moved pigs well away from homes and major drainage works on most islands have reduced breeding sites for mosquitoes.2
More recently a small outbreak of JE has occurred in Australia, with cases of JE in humans notified in Victoria, NSW, Queensland, South Australia and the Norther Territory.4
A systematic review published in 2011 World Health Organisation (WHO) bulletin, estimated that globally approximately 67,900 JE cases typically occur annually in the 24 JE-endemic countries, for an overall incidence of 1.8 per 100,000. Of which, only about 10% are reported to the WHO.4
Treatment
There is no specific treatment for JE; clinical management is supportive. Patients with severe meningeal symptoms often require pain control for headaches and antiemetic therapy and rehydration for associated nausea and vomiting. Patients with encephalitis require close monitoring for the development of elevated intracranial pressure, seizures, and inability to protect their airway.1
Featured content

Register to receive full access (Healthcare Professionals Only)
Are you a registered healthcare professional?
Register in less than a minute to access the latest updates and resources to support your practice and help deliver better outcomes for your patients.
Can’t find what you’re looking for?
Search our extensive Content Library
- Japanese Encephalitis. Centers for Disease Control and Prevention. www.cdc.gov/japaneseencephalitis/index.html. Accessed July 2024
- Australian Immunisation Handbook 10th edition. Australian Govt. Department of health. https://immunisationhandbook.health.gov.au/vaccine-preventable-diseases/japanese-encephalitis Accessed July 2024
- Japanese encephalitis virus – Protecting Australians from JEV Australian Government Department of Health and Age care https://www.health.gov.au/resources/publications/japanese-encephalitis-virus-protecting-australians-from-jev?language=en Accessed July 2024
- Campbell GL, Hills SL, Fischer M, et al. Estimated global incidence of Japanese encephalitis: a systematic review. Bulletin of the World Health Organization. 2011;89:766-774E.
MAT-AU-2101887 - 2.0 - 07/2024
Waddling-Gait---Robert,-28-year-old-mild-LOPD-patient
Waddling Gait - Robert, 28-year-old mild LOPD patient
Reaching-Overhead---Robert,-28-year-old-mild-LOPD-patient
Reaching Overhead - Robert, 28-year-old mild LOPD patient
Standing-From-Sitting---Robert,-28-year-old-mild-LOPD-patient
Standing From Sitting - Robert, 28-year-old mild LOPD patient
Climbing-Stairs---Robert,-28-year-old-mild-LOPD-patient
Climbing Stairs - Robert, 28-year-old mild LOPD patient
Waddling-Gait---Karen,-18-year-old-moderate-LOPD-patient

Waddling Gait - Karen, 18-year-old moderate LOPD patient
Reaching-Overhead---Karen,-18-year-old-moderate-LOPD-patient

Reaching Overhead - Karen, 18-year-old moderate LOPD patient
Standing-From-Sitting---Karen,-18-year-old-moderate-LOPD-patient

Standing From Sitting - Karen, 18-year-old moderate LOPD patient
Climbing-Stairs---Karen,-18-year-old-moderate-LOPD-patient

Climbing Stairs - Karen, 18-year-old moderate LOPD patient
ASPIRE-ICT-1-23_Harrington_MAT-AU-2302788-1

ASPIRE-ICT-1-23_Kyle-Blakey_MAT-AU-2302789-1

Which-biologic-and-why--When-to-switch-to-another-one-

Waddling-Gait---Brian,-44-year-old-severe-LOPD-patient

Waddling Gait - Brian, 44-year-old severe LOPD patient
Reaching-Overhead---Brian,-44-year-old-severe-LOPD-patient

Reaching Overhead - Brian, 44-year-old severe LOPD patient
Standing-From-Sitting---Brian,-44-year-old-severe-LOPD-patient

Standing From Sitting - Brian, 44-year-old severe LOPD patient
Climbing-Stairs---Brian,-44-year-old-severe-LOPD-patient

Climbing Stairs - Brian, 44-year-old severe LOPD patient
RESP-ICT2_Wark_MAT-AU-2301970
.webp/jcr:content/RESP-ICT2-Wark_400X300%20(1).webp)
RESP-ICT2_Wark_MAT-AU-2301970
RESP-ICT2_Stone_MAT-AU-2301972
.webp/jcr:content/RESP-ICT2-Stone_400X300%20(1).webp)
RESP-ICT2_Stone_MAT-AU-2301972
Remission-in-rheumatology---Dr-Michelle-Tellus
.webp/jcr:content/RESP-ICT2-Tellus_400X300%20(1).webp)
Remission in rheumatology - Dr Michelle Tellus
Pavord_MAT-AU-2300571

Pavord_MAT-AU-2300571
Wark_MAT-AU-2300572

Wark_MAT-AU-2300572
Q-A-Discussion_MAT-AU-2300573

Q&A-Discussion_MAT-AU-2300573
RESP-ICT3_Tellus_MAT-AU-2302033

RESP-ICT3_Tellus_MAT-AU-2302033
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Hew_MAT-AU-2302035

RESP-ICT3_Hew_MAT-AU-2302035
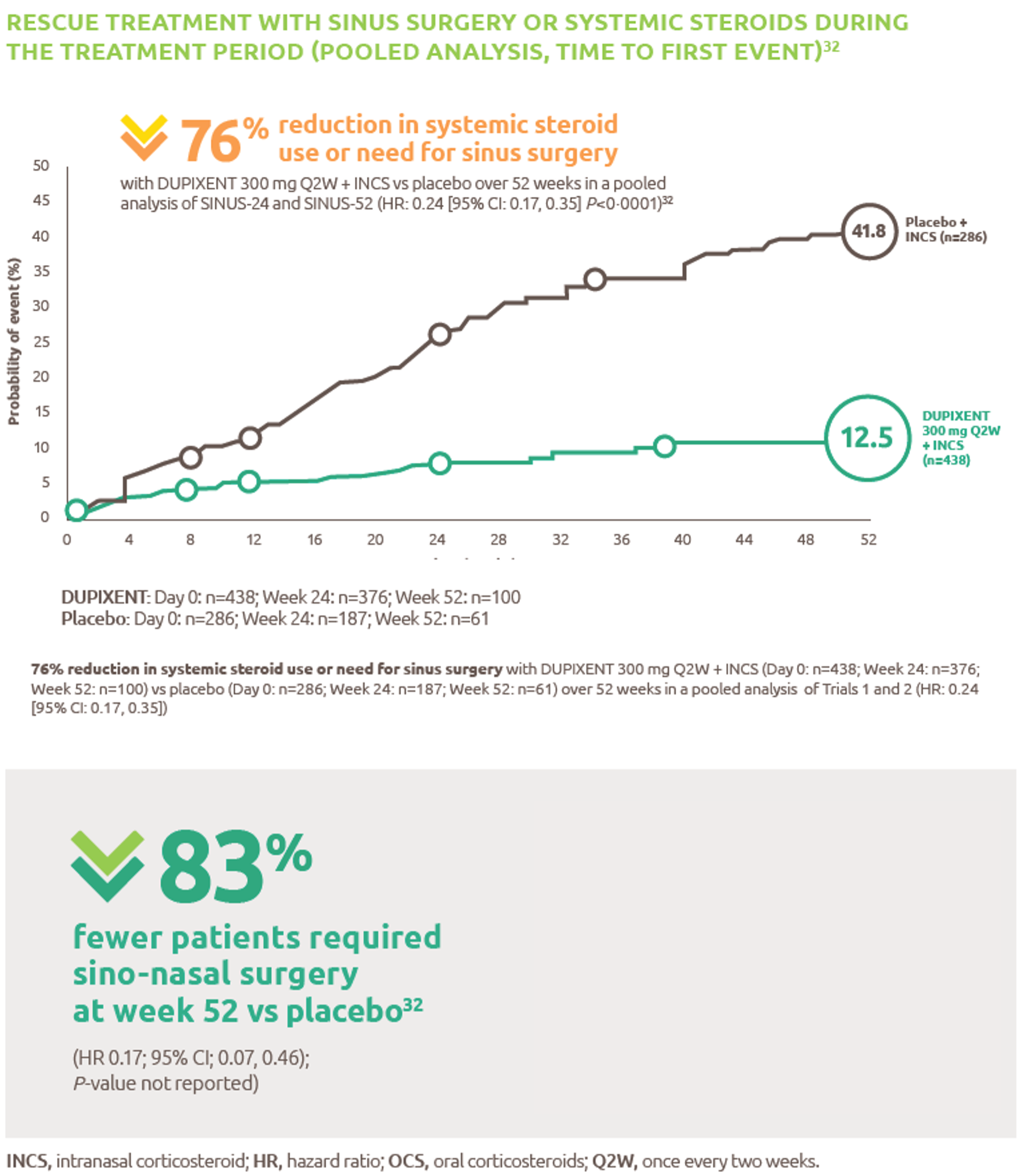
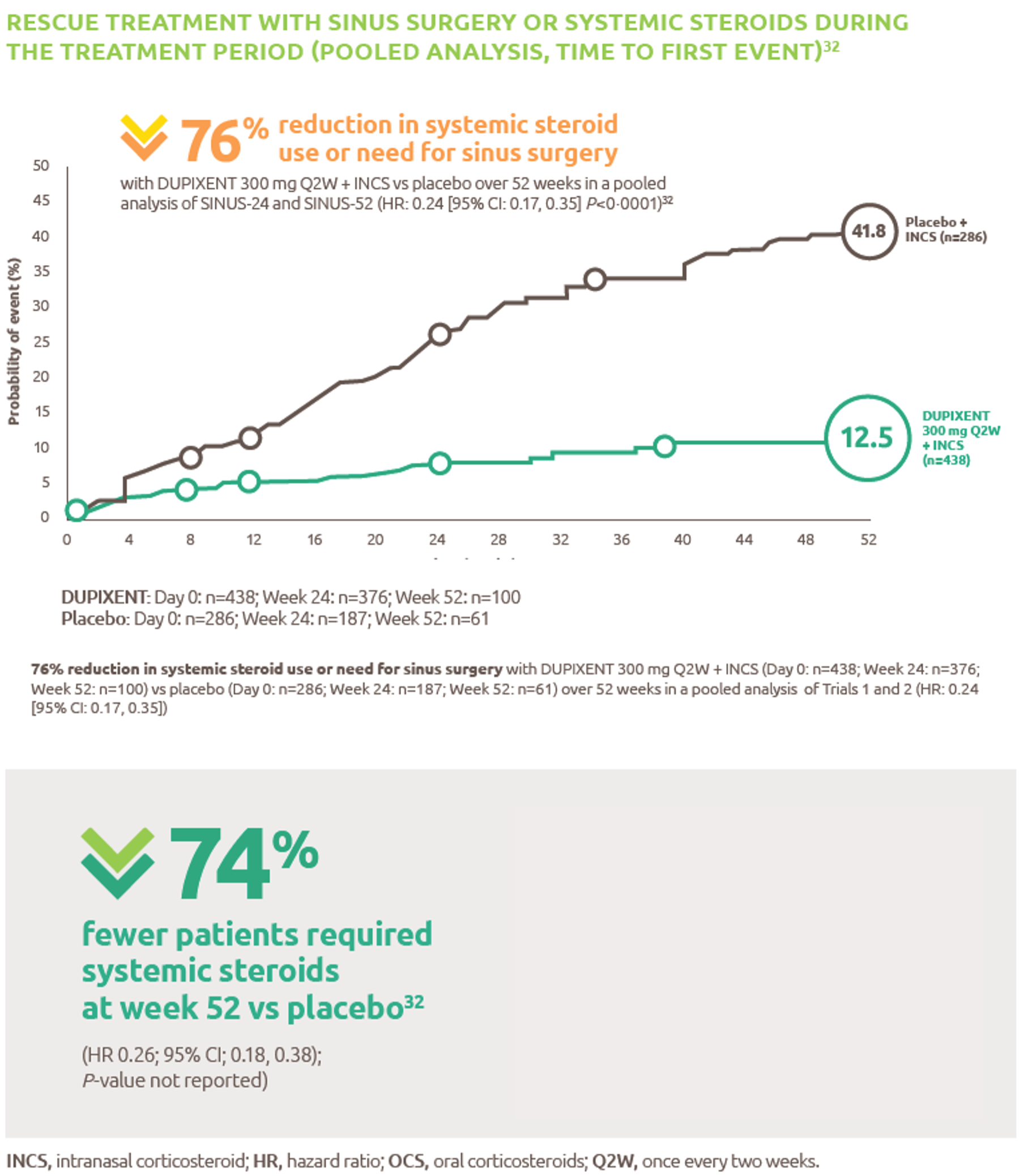
Reduced-need-for-sinus-surgery
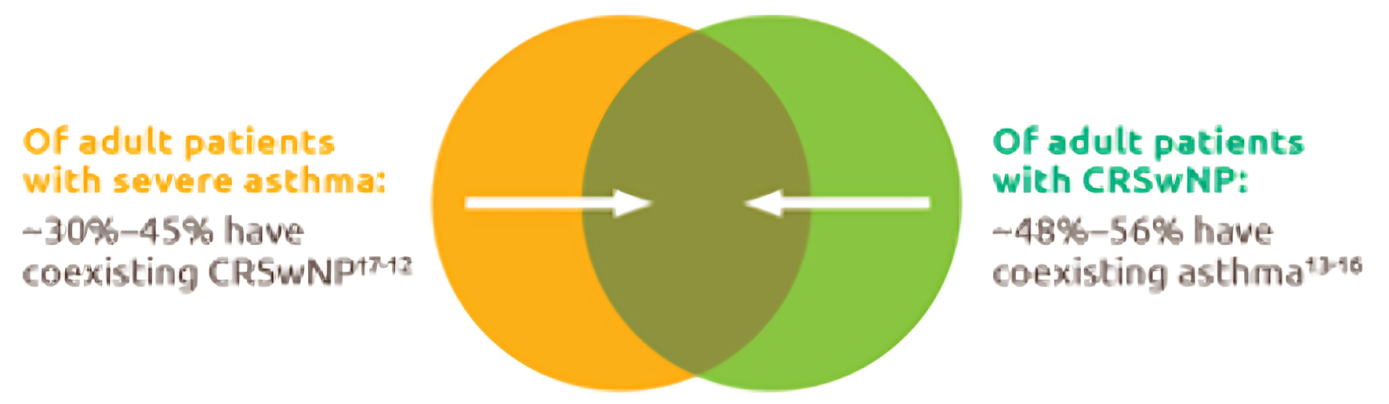
Up-to-45--of-severe-asthma-patients-have-comorbid-CRSwNP
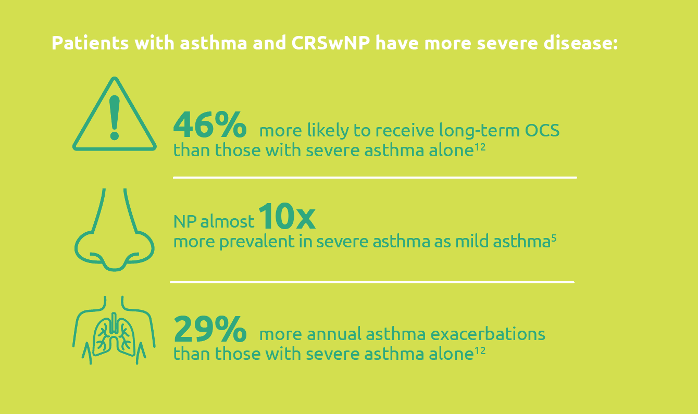
Severe-asthma-with-comorbid-CRSwNP-leads-to-more-severe-disease
.png)
Less-rescue-oral-corticosteriod-use
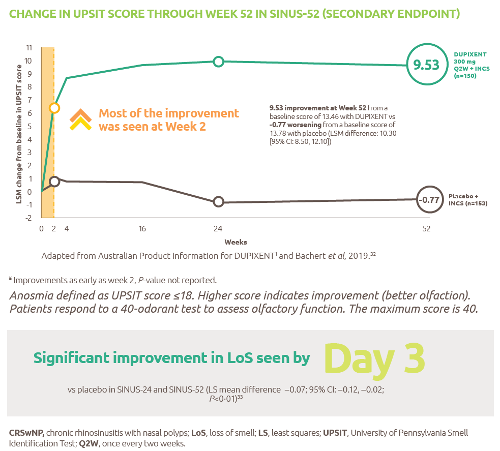
Improved-sense-of-smell
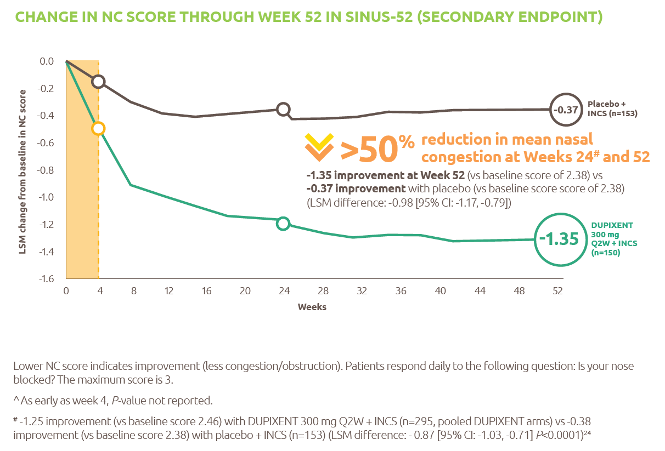
Reduced-obstruction-and-congestion
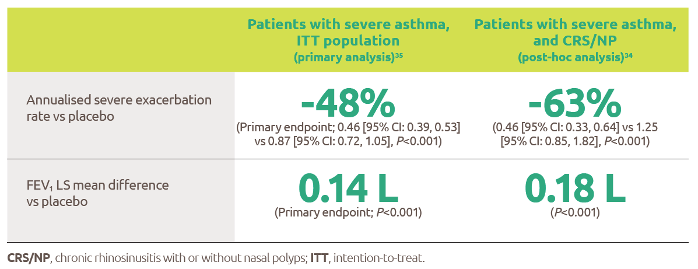
Reduced-asthma-exacerbations-and-improved-lung-function
IL-4-and-IL-13-are-key-and-central-drivers-of-type-2-inflammation

Gaucher-diagnosis-1

RESP-ICT2_Debate_MAT-AU-2301973

RESP-ICT2_Debate_MAT-AU-2301973
RESP-ICT3_Q-A_MAT-AU-2302036

RESP-ICT3_Q&A_MAT-AU-2302036
ASPIRE-ICT1-23_Q-A_MAT-AU-2302791-1

RESP-ICT2_Stone_CS_MAT-AU-2301975

RESP-ICT2_Stone_CS_MAT-AU-2301975
RESP-ICT2_Wark_CS_MAT-AU-2301974

RESP-ICT2_Wark_CS_MAT-AU-2301974
RESP-ICT2_Panel-Discussion_MAT-AU-2301976

RESP-ICT2_Panel-Discussion_MAT-AU-2301976
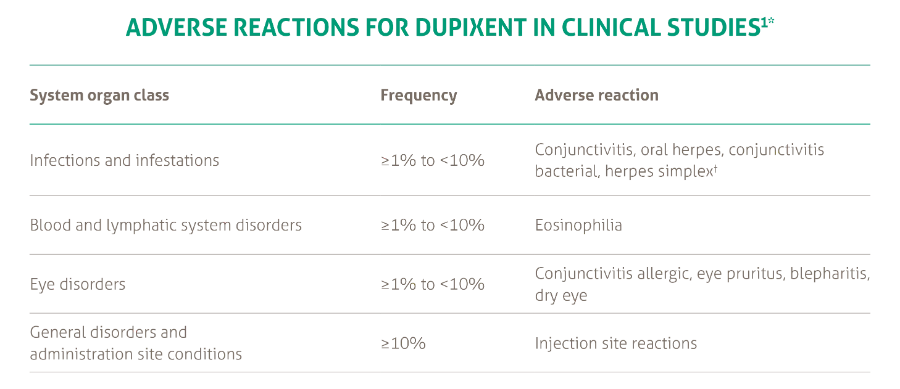
SANA7993_Safety-Page-Tables_V0.2_1_New3
Products_Dermatology_Atopic-Dermatitis_Adverse-Events-Adults_18012021