.png/jcr:content.png)
Cholera
Discover timely medical updates and key resources on preventing and controlling cholera – helping you stay informed and improve patient outcomes.
*Image is not an actual patient.
About cholera
The challenges of cholera
Cholera is an acute, diarrhoeal illness caused by infection of the intestine with the bacterium Vibrio cholerae and is spread by ingestion of contaminated food or water. The infection is often mild or without symptoms, but can sometimes be severe. Approximately 1 in 10 infected persons have severe disease. In these people, rapid loss of body fluids leads to dehydration and shock. Without treatment, death can occur within hours.1
Supporting cholera management through information
Effective management of cholera involves a comprehensive understanding of the condition. For healthcare professionals, staying informed about the disease and evolving patient needs is crucial for providing care.
To foster a broader understanding of cholera, this page offers a range of selected materials and information.
Understanding cholera research and care
Cholera is an acute diarrheal infection caused by the bacterium Vibrio cholerae. Global research aims to better understand, treat, and prevent it, ultimately seeking to control outbreaks and improve public health. Broad areas of focus in cholera research often include:
- Understanding disease transmission and epidemiology
- Advancing prevention strategies, including vaccination
- Improving case management and supportive care
- Addressing public health interventions and access
Signs and symptoms
The incubation period for the cholera is 12 hours to 5 days. Most people infected with V. cholerae do not develop any symptoms, although the bacteria are present in their faeces for 1-10 days after infection and are shed back into the environment, potentially infecting other people. Of those who develop symptoms, these are mild to moderate and can be treated with oral rehydration fluids.2
However, others will develop acute watery diarrhoea (also called ‘rice water stools’) with severe dehydration which can lead to death if untreated. Other symptoms of severe disease include vomiting, tachycardia, loss of skin elasticity, low blood pressure, muscle cramps, restlessness or irritability.1
Diagnosis
It is almost impossible to distinguish a single patient with cholera from a patient infected by another pathogen that causes acute watery diarrhoea without testing a stool sample. Isolation and identification of Vibrio cholerae serogroup O1 or O139 by culture of a stool specimen remains the gold standard for the laboratory diagnosis of cholera. In areas with limited to no laboratory testing, the Crystal VC® dipstick rapid test can provide an early warning to public health officials that an outbreak of cholera is occurring. However, due to low sensitivity and specificity of the test, it should be confirmed using traditional culture-based methods suitable for the isolation and identification of V. cholerae.1
Prevention
A combination of surveillance, provision of safe water, sanitation and hygiene promotion and oral cholera vaccines are used to prevent the disease.2 Vaccination against cholera is not an official requirement for entry into any foreign country. Cholera vaccination is not routinely recommended as the risk to travellers is very low, despite the endemicity of cholera in some countries often visited by Australians. Careful and sensible selection of food and water is of far greater importance to the traveller than cholera vaccination.3
An oral cholera vaccine is available in Australia for adults and children aged 2 years and older, and should be considered for the following travellers:3
- travellers with a high risk of exposure, including, humanitarian aid workers deployed where there is an endemic outbreak of cholera
- travellers to areas where cholera exists who have a high risk of acquiring diarrhoeal disease due to an underlying medical condition (eg. achlorhydria)
- travellers to areas where cholera exists who have a higher risk of severe complications from diarrhoeal disease (eg. inflammatory bowel disease, poorly controlled or complicated diabetes, HIV or other immunocompromising conditions, significant cardiovascular disease).
Bacteriology
Vibrio cholerae is a motile, curved gram-negative bacillus with more than 150 serogroups based on differences in the O antigens. Cholera is caused by enterotoxin-producing V. cholerae of serogroups O1 and O139. The bacteria can survive under unfavourable conditions in a viable dormant state and are transmitted predominantly by ingestion of faecally contaminated food or water.3 Only toxigenic strains of serogroups O1 and O139 have caused widespread epidemics and are reportable to the WHO as “cholera”. Serogroup O1 includes two biotypes (classical and El Tor), each of which includes two distinct serotypes, Inaba and Ogawa.1
Epidemiology
Cholera can be endemic or epidemic. A cholera outbreak/epidemic can occur in both endemic countries and in countries where cholera does not regularly occur.2 It is considered endemic in Haiti, south and south-east Asia and sub-saharan Africa.3
Almost all the cases of cholera reported in Australia (about 2 to 6 cases a year) occur in individuals who have been infected in endemic areas overseas. In 1977, a locally acquired case led to the discovery of V. cholerae in some rivers of the Queensland coast , which indicated that health workers should be aware that sporadic cases may occur rarely following contact with estuarine waters. All cases of cholera reported since the commencement of the National Notifiable Diseases Surveillance System in 1991 have been acquired outside Australia, except for 1 case in 1996 which was laboratory-acquired and 3 cases in 2006 reported in Sydney, which were associated with consumption of raw imported whitebait in patients who had no history of recent travel to known cholera-endemic areas.3
Treatment
The majority of people who develop cholera can be treated successfully through prompt administration of oral rehydration solution (ORS). Severely dehydrated patients are at risk of shock and require the rapid administration of intravenous fluids. These patients are also given appropriate antibiotics to diminish the duration of diarrhoea, reduce the volume of rehydration fluids needed, and shorten the amount and duration of V. cholerae excretion in their stool.2
Resources and tools

Register to receive full access (Healthcare Professionals Only)
Are you a registered healthcare professional?
Register in less than a minute to access the latest updates and resources to support your practice and help deliver better outcomes for your patients.
Can’t find what you’re looking for?
Search our extensive Content Library
- Cholera. Centers for Disease Control and Prevention. www.cdc.gov/cholera/index.html. (Accessed August 2021)
Waddling-Gait---Robert,-28-year-old-mild-LOPD-patient
Waddling Gait - Robert, 28-year-old mild LOPD patient
Reaching-Overhead---Robert,-28-year-old-mild-LOPD-patient
Reaching Overhead - Robert, 28-year-old mild LOPD patient
Standing-From-Sitting---Robert,-28-year-old-mild-LOPD-patient
Standing From Sitting - Robert, 28-year-old mild LOPD patient
Climbing-Stairs---Robert,-28-year-old-mild-LOPD-patient
Climbing Stairs - Robert, 28-year-old mild LOPD patient
Waddling-Gait---Karen,-18-year-old-moderate-LOPD-patient

Waddling Gait - Karen, 18-year-old moderate LOPD patient
Reaching-Overhead---Karen,-18-year-old-moderate-LOPD-patient

Reaching Overhead - Karen, 18-year-old moderate LOPD patient
Standing-From-Sitting---Karen,-18-year-old-moderate-LOPD-patient

Standing From Sitting - Karen, 18-year-old moderate LOPD patient
Climbing-Stairs---Karen,-18-year-old-moderate-LOPD-patient

Climbing Stairs - Karen, 18-year-old moderate LOPD patient
ASPIRE-ICT-1-23_Harrington_MAT-AU-2302788-1

ASPIRE-ICT-1-23_Kyle-Blakey_MAT-AU-2302789-1

Which-biologic-and-why--When-to-switch-to-another-one-

Waddling-Gait---Brian,-44-year-old-severe-LOPD-patient

Waddling Gait - Brian, 44-year-old severe LOPD patient
Reaching-Overhead---Brian,-44-year-old-severe-LOPD-patient

Reaching Overhead - Brian, 44-year-old severe LOPD patient
Standing-From-Sitting---Brian,-44-year-old-severe-LOPD-patient

Standing From Sitting - Brian, 44-year-old severe LOPD patient
Climbing-Stairs---Brian,-44-year-old-severe-LOPD-patient

Climbing Stairs - Brian, 44-year-old severe LOPD patient
RESP-ICT2_Wark_MAT-AU-2301970
.webp/jcr:content/RESP-ICT2-Wark_400X300%20(1).webp)
RESP-ICT2_Wark_MAT-AU-2301970
RESP-ICT2_Stone_MAT-AU-2301972
.webp/jcr:content/RESP-ICT2-Stone_400X300%20(1).webp)
RESP-ICT2_Stone_MAT-AU-2301972
Remission-in-rheumatology---Dr-Michelle-Tellus
.webp/jcr:content/RESP-ICT2-Tellus_400X300%20(1).webp)
Remission in rheumatology - Dr Michelle Tellus
Pavord_MAT-AU-2300571

Pavord_MAT-AU-2300571
Wark_MAT-AU-2300572

Wark_MAT-AU-2300572
Q-A-Discussion_MAT-AU-2300573

Q&A-Discussion_MAT-AU-2300573
RESP-ICT3_Tellus_MAT-AU-2302033

RESP-ICT3_Tellus_MAT-AU-2302033
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Hew_MAT-AU-2302035

RESP-ICT3_Hew_MAT-AU-2302035
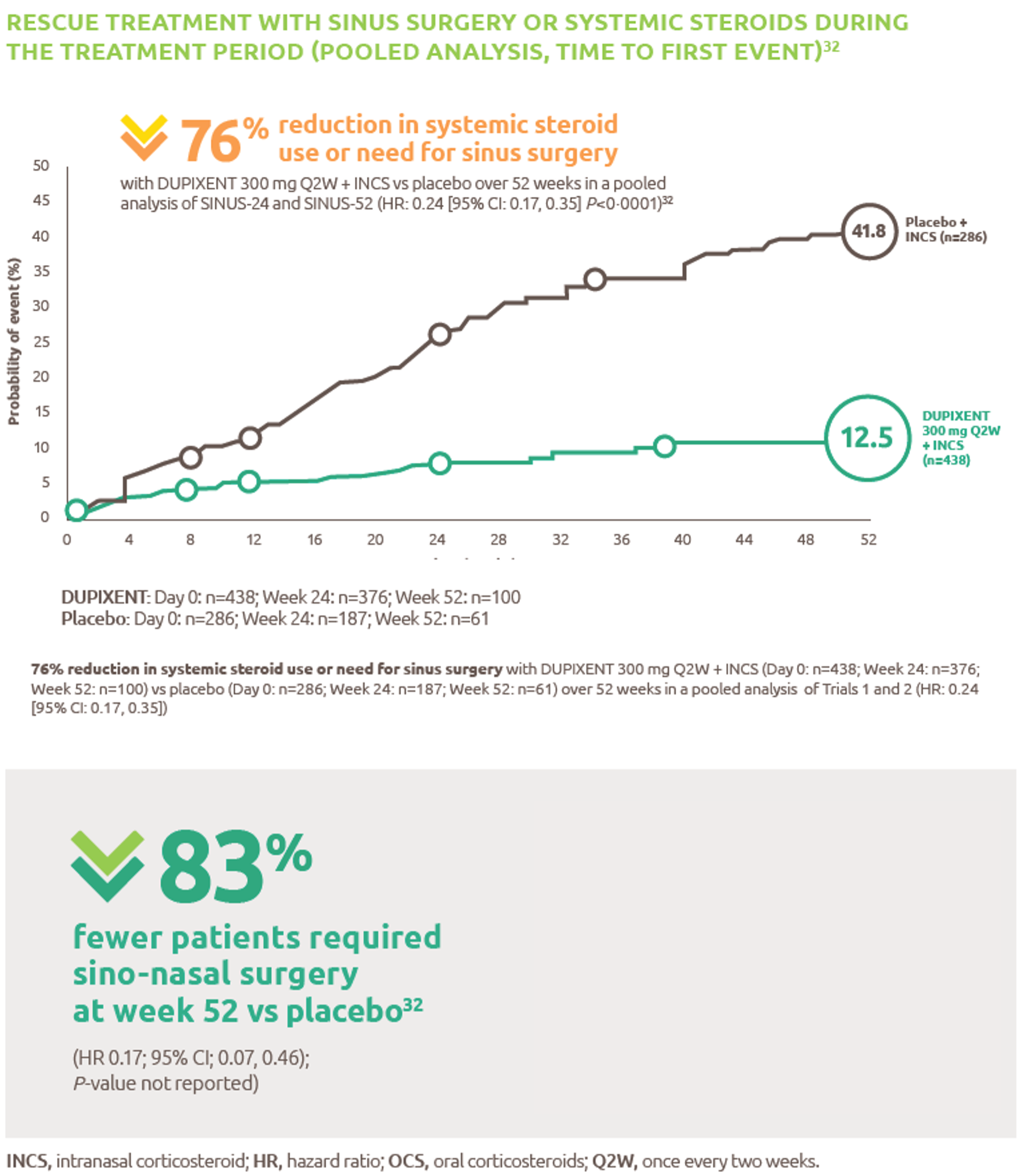
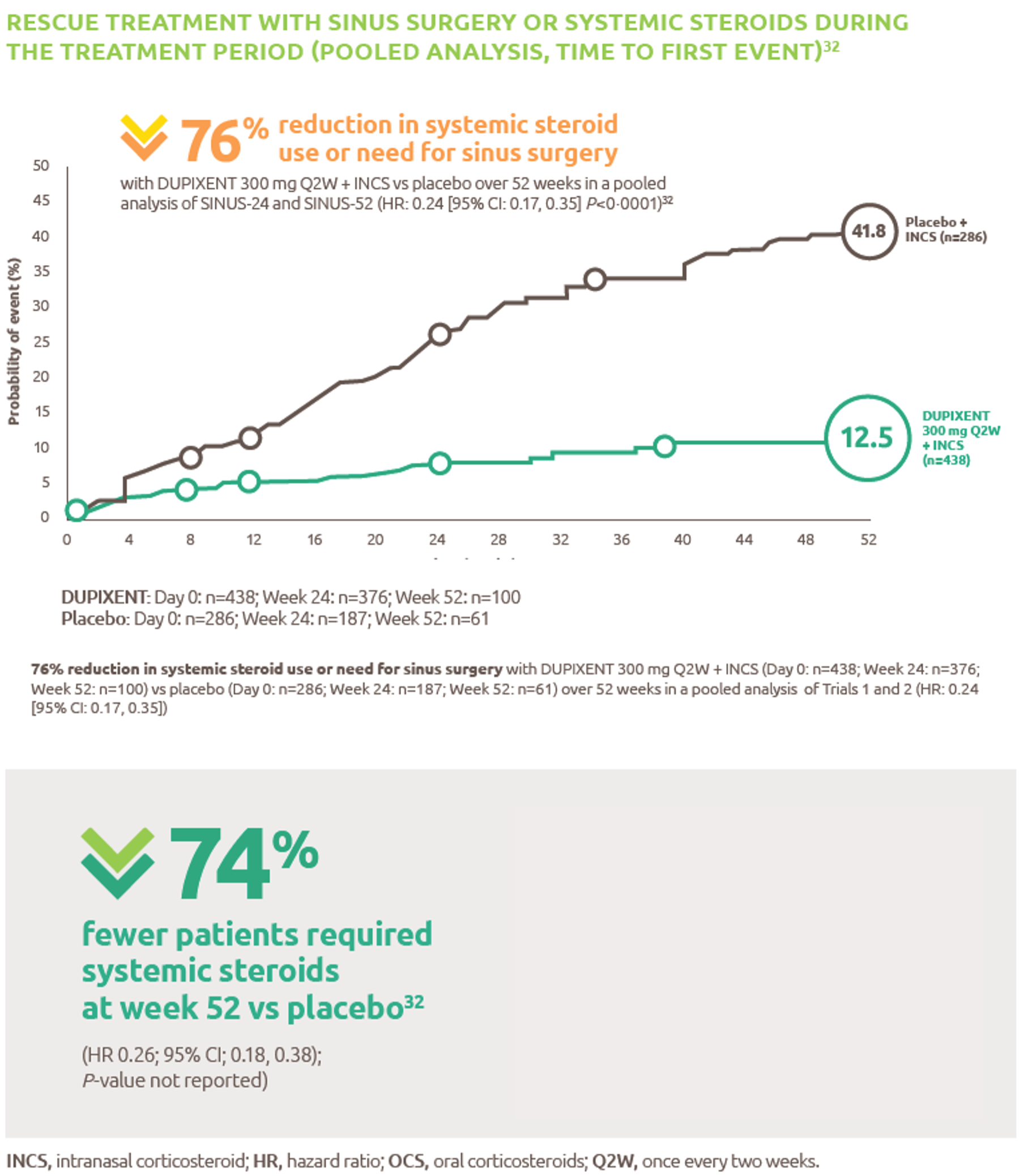
Reduced-need-for-sinus-surgery
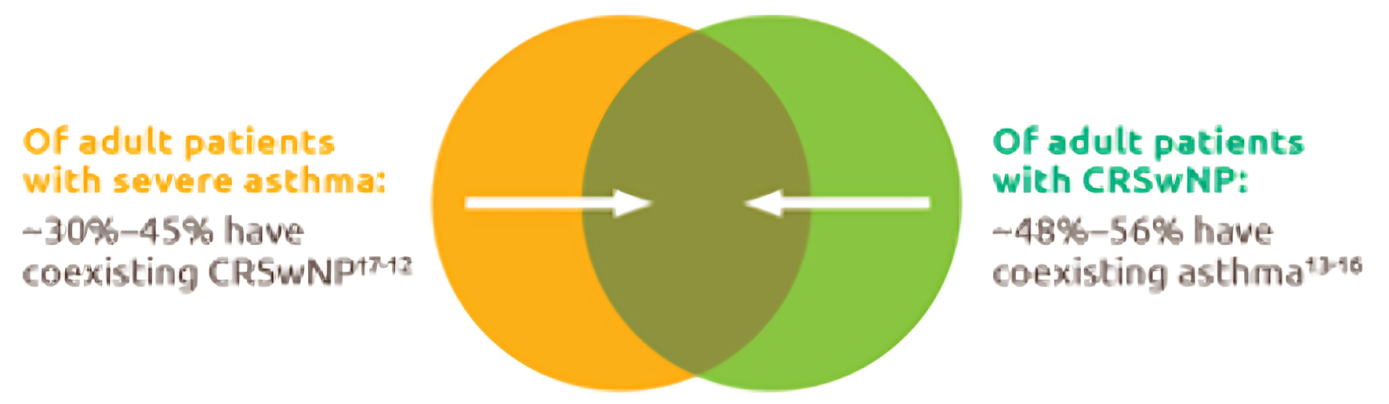
Up-to-45--of-severe-asthma-patients-have-comorbid-CRSwNP
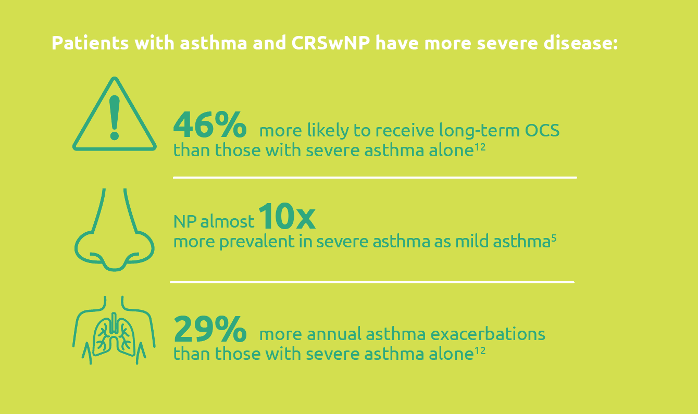
Severe-asthma-with-comorbid-CRSwNP-leads-to-more-severe-disease
.png)
Less-rescue-oral-corticosteriod-use
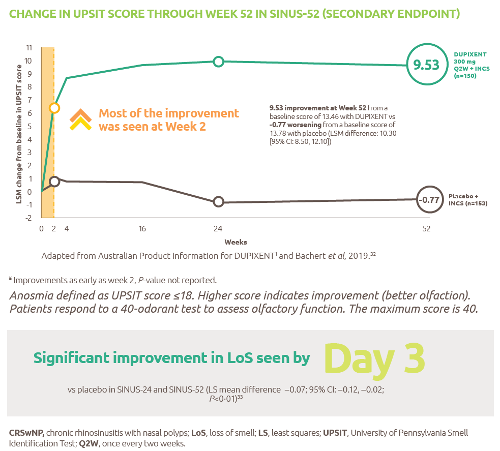
Improved-sense-of-smell
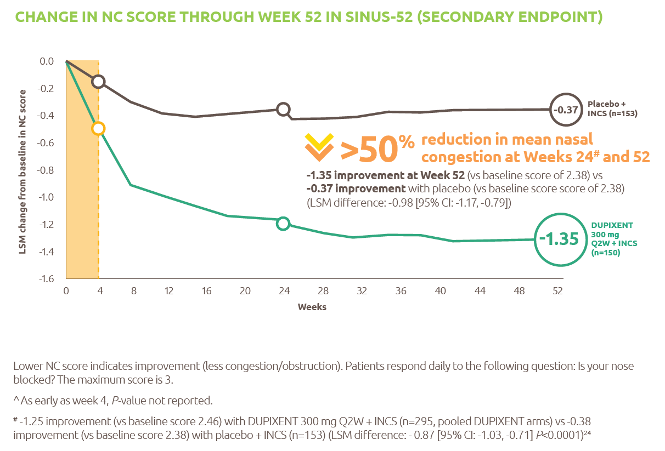
Reduced-obstruction-and-congestion
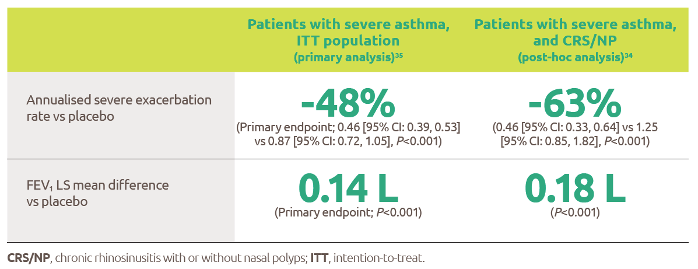
Reduced-asthma-exacerbations-and-improved-lung-function
IL-4-and-IL-13-are-key-and-central-drivers-of-type-2-inflammation

Gaucher-diagnosis-1

RESP-ICT2_Debate_MAT-AU-2301973

RESP-ICT2_Debate_MAT-AU-2301973
RESP-ICT3_Q-A_MAT-AU-2302036

RESP-ICT3_Q&A_MAT-AU-2302036
ASPIRE-ICT1-23_Q-A_MAT-AU-2302791-1

RESP-ICT2_Stone_CS_MAT-AU-2301975

RESP-ICT2_Stone_CS_MAT-AU-2301975
RESP-ICT2_Wark_CS_MAT-AU-2301974

RESP-ICT2_Wark_CS_MAT-AU-2301974
RESP-ICT2_Panel-Discussion_MAT-AU-2301976

RESP-ICT2_Panel-Discussion_MAT-AU-2301976
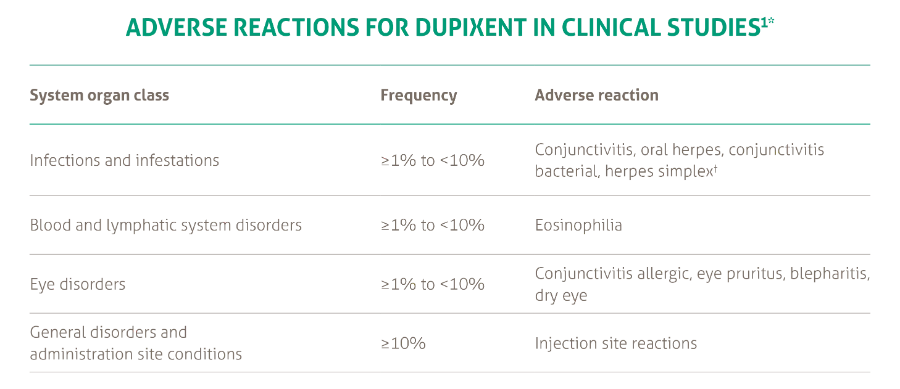
SANA7993_Safety-Page-Tables_V0.2_1_New3
Products_Dermatology_Atopic-Dermatitis_Adverse-Events-Adults_18012021