Haemophilus influenzae type b (Hib)
Discover timely medical updates and key resources on preventing and controlling haemophilus influenzae type B (Hib) – helping you stay informed and improve patient outcomes.
*Image is not an actual patient.
About Hib
The challenges of Hib
Haemophilus influenzae type b (Hib) is a bacterium responsible for severe pneumonia, meningitis and other invasive diseases almost exclusively in children aged less than 5 years. It is transmitted through the respiratory tract from infected to susceptible individuals. Vaccines are the only public health tool capable of preventing the majority of serious Hib disease.1
Don’t miss these key links
Signs and symptoms
Invasive Hib disease presents most frequently as meningitis (approximately 50%–65% of invasive Hib infections), but may also present as bacteraemic pneumonia, bacteraemia, cellulitis, epiglottitis, septic arthritis, osteomyelitis and pericarditis. Diseases caused by direct spread from the nasopharynx are usually considered non-invasive and include non-bacteraemic pneumonia, otitis media, sinusitis and conjunctivitis.1
The incubation period ranges between 2 to 10 days. Most common symptoms of Hib meningitis are acute onset of fever, headache, seizures and one or more of the following signs: neck stiffness, altered consciousness or other meningeal signs (e.g. photophobia).1
In infants <6 months of age, the signs and symptoms may be non-specific but often include a bulging fontanelle. Even with adequate medical treatment, 5% of children with Hib meningitis die and 20%–40% of survivors suffer severe sequelae including blindness, deafness, and learning disabilities. Symptoms of Hib pneumonia include cough, fever, rapid breathing (>40 breaths per minute) and lower chest wall in-drawing.1
Symptoms of acute epiglottitis include high fever, sore throat, difficulty in swallowing and stridor. It may lead to acute respiratory obstruction. This form of Hib disease was common in older children in North America and Europe in the pre-vaccination era; it is rarely reported from developing countries where Hib disease occurs in younger children.1
Diagnosis
Hib meningitis and pneumonia cannot be differentiated from meningitis and pneumonia caused by other bacterial pathogens on clinical examination alone. In clinically suspected Hib meningitis the etiological diagnosis can be achieved by: isolating Hib from cerebrospinal fluid (CSF); a positive latex agglutination or polymerase chain reaction (PCR) test for Hib from CSF; finding purulent CSF with a gram stain showing gram negative coccobacilli; or by growth of Hib from blood cultures. Infection in other sites may be proven through demonstration of Hib or Hib-specific components in the affected body fluid or tissue. It is difficult to identify the bacterial etiology of pneumonia. Blood cultures and cultures of lung aspirates are accurate way of identifying a bacterial agent as a cause of pneumonia.1
Prevention
Hib infections can be prevented through vaccination. The following types of Hib vaccines are available in Australia:
- Monovalent Hib vaccines
- Hexavalent combination vaccines which contain Hib in combination with diphtheria, tetanus, pertussis, poliovirus and hepatitis B antigens
Bacteriology
Haemophilus influenzae is a Gram-negative coccobacillus that is a normal part of upper respiratory tract flora. It can be isolated in two forms: capsular and non-capsular. Strains isolated from respiratory tract specimens (sputum, middle ear or sinus fluid) are non-capsular and are known as non-typeable Haemophilus influenzae (NTHi). Six capsular types (a to f) have been described and, before the introduction of vaccination against Haemophilus influenzae type b (Hib), almost all H. influenzae isolates from sterile sites (blood, cerebrospinal fluid, joint or pleural fluid) were of the b capsular type.2
Epidemiology
Hib was previously the commonest cause of bacterial meningitis in Australian children. Aboriginal and Torres Strait Islander children, especially in remote and rural areas, had a much higher incidence of Hib infection and presented at a younger age than non-Indigenous children. Hib epiglottitis was particularly rare among Indigenous children.3
In Australia, Hib conjugate vaccines were first introduced into the routine vaccination schedule in 1993, leading to a more than 95% reduction in the reported incidence of Hib disease. Introduction of Hib conjugate vaccines into routine vaccination programs has led to a dramatic decline in the incidence of Hib disease in many regions of the world.3
The sharp decline in Hib disease incidence since then is seen both among the Indigenous and non-Indigenous populations. In the pre-vaccination era, there were at least 500 cases of Hib disease and 10–15 deaths annually among Australian children aged <6 years. At present, the number of cases reported in Australia for all ages is around 20 per year, a reduction of over 95% from the pre-vaccination period.3
Treatment
Hib disease is treated with appropriate antibiotics (including ampicillin or 3rd generation cephalosporins like ceftriaxone and cefotaxime for meningitis, oral amoxicillin for non-immunocompromised children aged 2–59 months with pneumonia, parenteral ampicillin and gentamicin for immunocompromised children and those presenting with severe pneumonia), symptomatic treatment, and supportive treatment of sequelae (including oxygen for meningitis patients presenting with hypoxaemia and airway support for epiglottitis). The choice of therapy depends on the presentation of Hib disease and local patterns of antibiotic resistance.1
Featured products

Register to receive full access (Healthcare Professionals Only)
Are you a registered healthcare professional?
Register in less than a minute to access the latest updates and resources to support your practice and help deliver better outcomes for your patients.
Can’t find what you’re looking for?
Search our extensive Content Library
- Haemophilus influenzae type b (Hib) Vaccination World Health Organization (WHO) position paper- September 2013. WHO. Weekly epidemiological record No. 39. 2013; 88:413–428
- Australian Immunisation Handbook. Australian Government. Department of Health. Vaccines, dosage and administration | Haemophilus influenzae type b (Hib) | The Australian Immunisation Handbook (health.gov.au). Accessed June 2024
- NCIRS. Haemophilus influenzae type b vaccines for Australian children Fact Sheet. https://ncirs.org.au/sites/default/files/2023-06/Hib%20factsheet%20June%202023.pdf. Accessed June 2024
MAT-AU-2501356 - 1.0 - 07/2025
Waddling-Gait---Robert,-28-year-old-mild-LOPD-patient
Waddling Gait - Robert, 28-year-old mild LOPD patient
Reaching-Overhead---Robert,-28-year-old-mild-LOPD-patient
Reaching Overhead - Robert, 28-year-old mild LOPD patient
Standing-From-Sitting---Robert,-28-year-old-mild-LOPD-patient
Standing From Sitting - Robert, 28-year-old mild LOPD patient
Climbing-Stairs---Robert,-28-year-old-mild-LOPD-patient
Climbing Stairs - Robert, 28-year-old mild LOPD patient
Waddling-Gait---Karen,-18-year-old-moderate-LOPD-patient

Waddling Gait - Karen, 18-year-old moderate LOPD patient
Reaching-Overhead---Karen,-18-year-old-moderate-LOPD-patient

Reaching Overhead - Karen, 18-year-old moderate LOPD patient
Standing-From-Sitting---Karen,-18-year-old-moderate-LOPD-patient

Standing From Sitting - Karen, 18-year-old moderate LOPD patient
Climbing-Stairs---Karen,-18-year-old-moderate-LOPD-patient

Climbing Stairs - Karen, 18-year-old moderate LOPD patient
ASPIRE-ICT-1-23_Harrington_MAT-AU-2302788-1

ASPIRE-ICT-1-23_Kyle-Blakey_MAT-AU-2302789-1

Which-biologic-and-why--When-to-switch-to-another-one-

Waddling-Gait---Brian,-44-year-old-severe-LOPD-patient

Waddling Gait - Brian, 44-year-old severe LOPD patient
Reaching-Overhead---Brian,-44-year-old-severe-LOPD-patient

Reaching Overhead - Brian, 44-year-old severe LOPD patient
Standing-From-Sitting---Brian,-44-year-old-severe-LOPD-patient

Standing From Sitting - Brian, 44-year-old severe LOPD patient
Climbing-Stairs---Brian,-44-year-old-severe-LOPD-patient

Climbing Stairs - Brian, 44-year-old severe LOPD patient
RESP-ICT2_Wark_MAT-AU-2301970
.webp/jcr:content/RESP-ICT2-Wark_400X300%20(1).webp)
RESP-ICT2_Wark_MAT-AU-2301970
RESP-ICT2_Stone_MAT-AU-2301972
.webp/jcr:content/RESP-ICT2-Stone_400X300%20(1).webp)
RESP-ICT2_Stone_MAT-AU-2301972
Remission-in-rheumatology---Dr-Michelle-Tellus
.webp/jcr:content/RESP-ICT2-Tellus_400X300%20(1).webp)
Remission in rheumatology - Dr Michelle Tellus
Pavord_MAT-AU-2300571

Pavord_MAT-AU-2300571
Wark_MAT-AU-2300572

Wark_MAT-AU-2300572
Q-A-Discussion_MAT-AU-2300573

Q&A-Discussion_MAT-AU-2300573
RESP-ICT3_Tellus_MAT-AU-2302033

RESP-ICT3_Tellus_MAT-AU-2302033
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Hew_MAT-AU-2302035

RESP-ICT3_Hew_MAT-AU-2302035
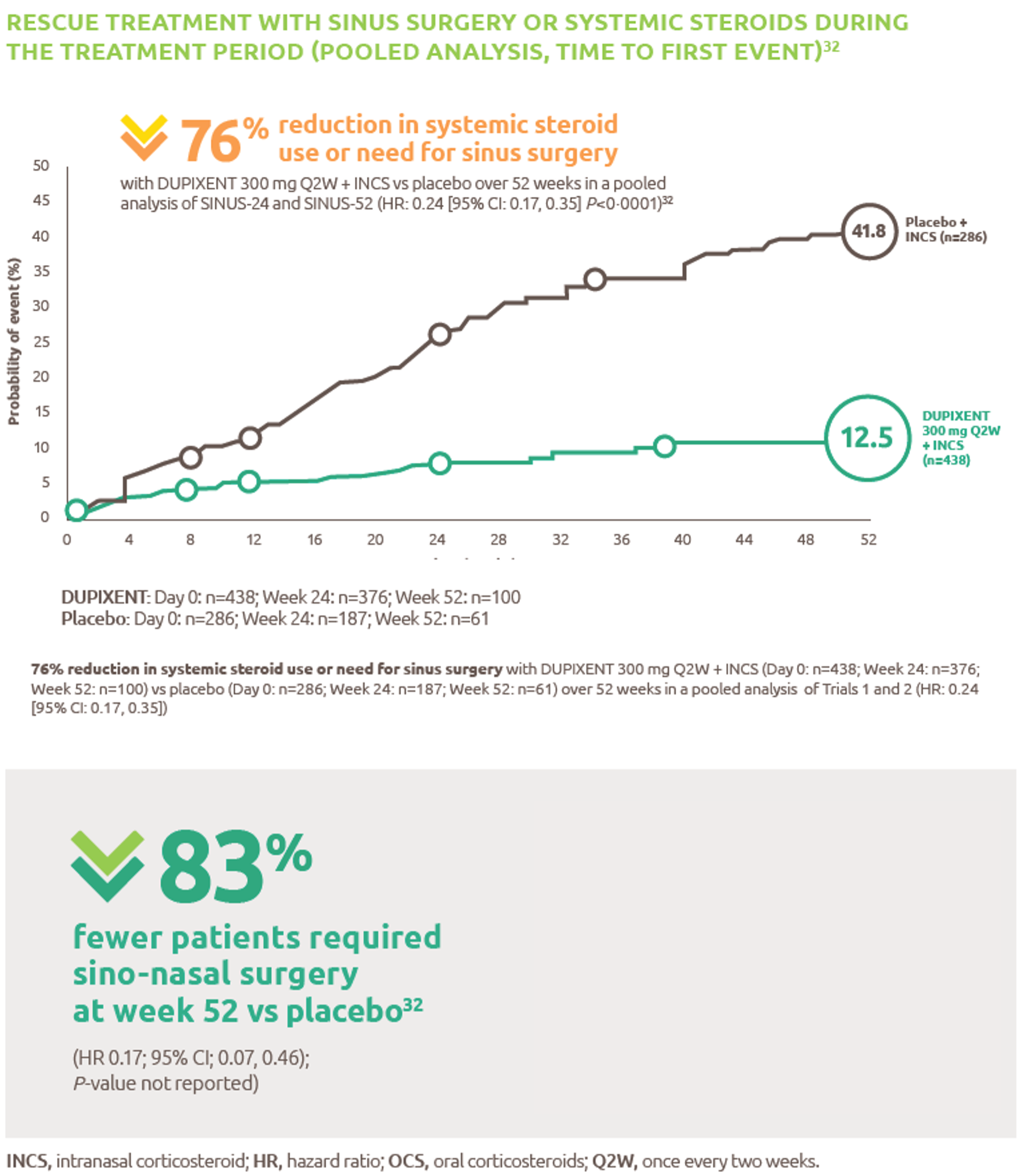
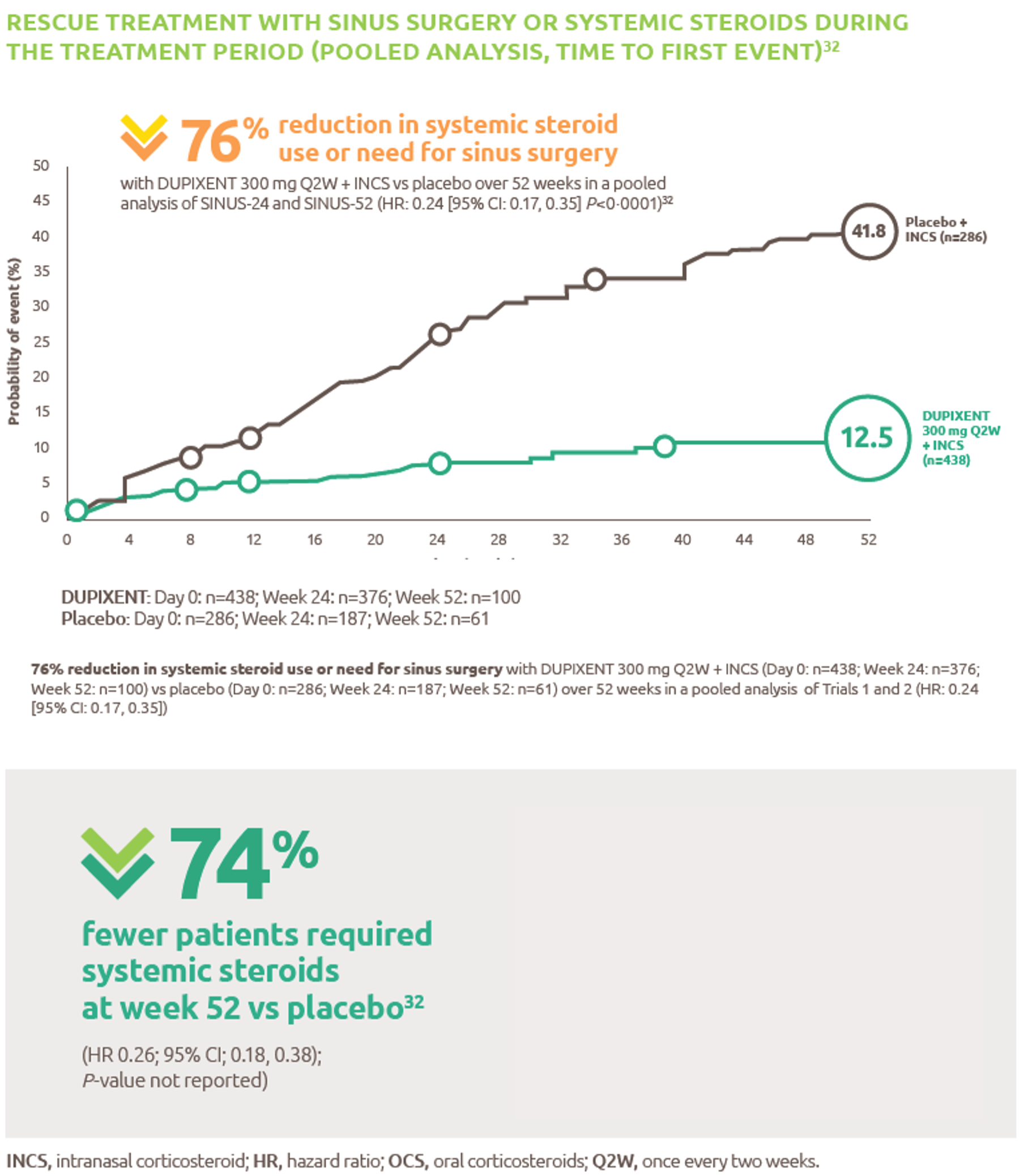
Reduced-need-for-sinus-surgery
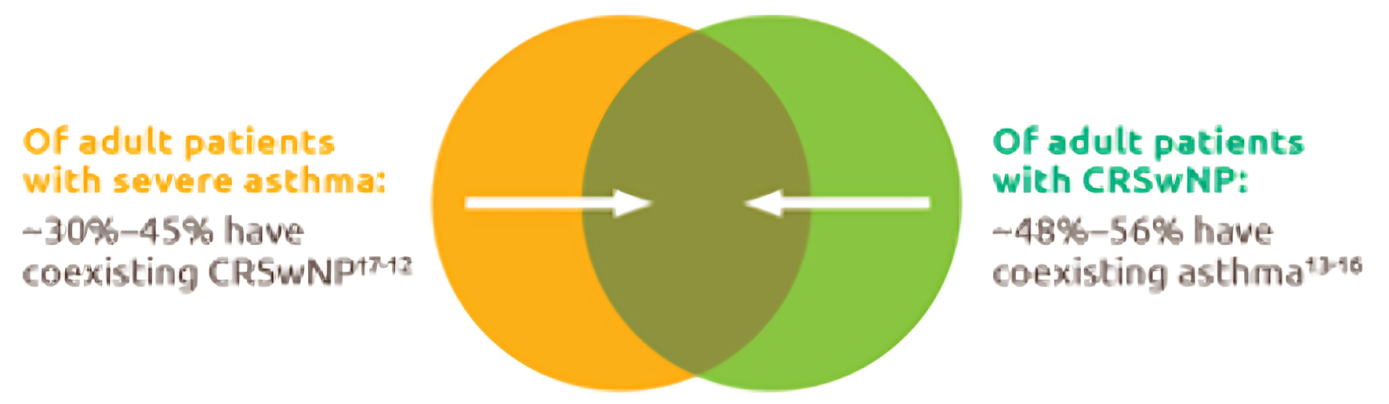
Up-to-45--of-severe-asthma-patients-have-comorbid-CRSwNP
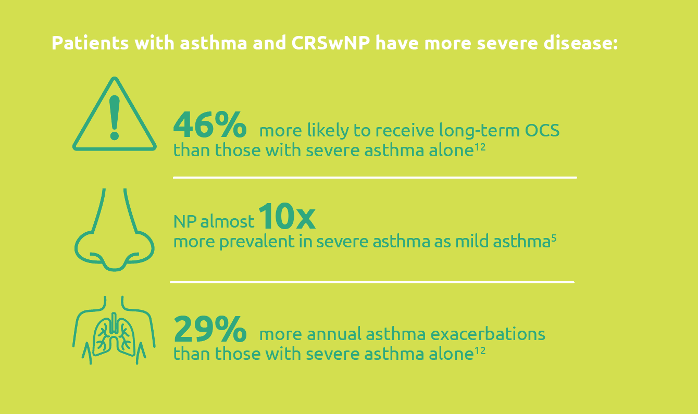
Severe-asthma-with-comorbid-CRSwNP-leads-to-more-severe-disease
.png)
Less-rescue-oral-corticosteriod-use
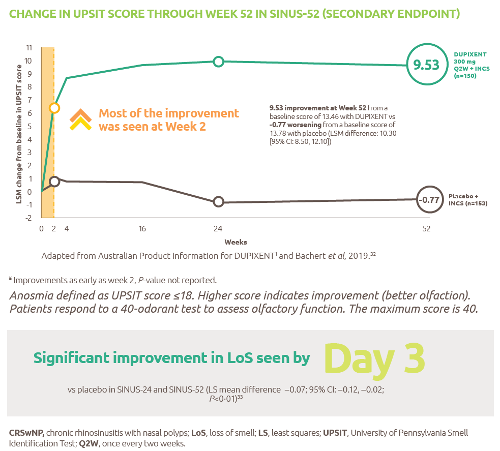
Improved-sense-of-smell
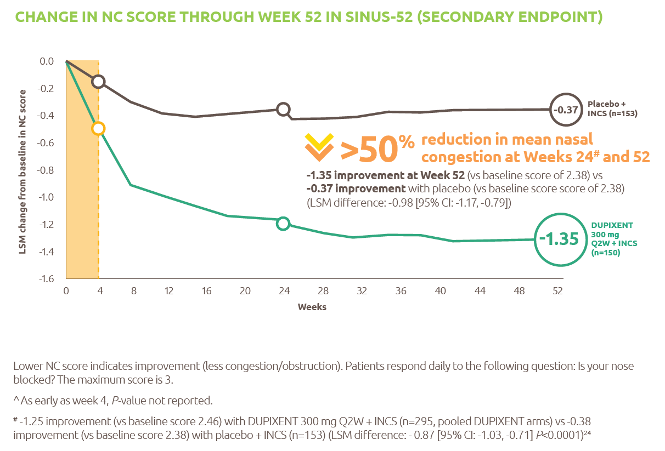
Reduced-obstruction-and-congestion
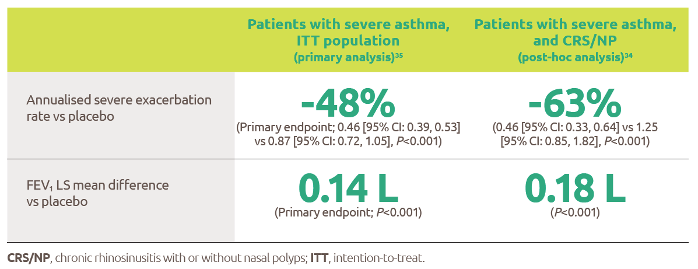
Reduced-asthma-exacerbations-and-improved-lung-function
IL-4-and-IL-13-are-key-and-central-drivers-of-type-2-inflammation

Gaucher-diagnosis-1

RESP-ICT2_Debate_MAT-AU-2301973

RESP-ICT2_Debate_MAT-AU-2301973
RESP-ICT3_Q-A_MAT-AU-2302036

RESP-ICT3_Q&A_MAT-AU-2302036
ASPIRE-ICT1-23_Q-A_MAT-AU-2302791-1

RESP-ICT2_Stone_CS_MAT-AU-2301975

RESP-ICT2_Stone_CS_MAT-AU-2301975
RESP-ICT2_Wark_CS_MAT-AU-2301974

RESP-ICT2_Wark_CS_MAT-AU-2301974
RESP-ICT2_Panel-Discussion_MAT-AU-2301976

RESP-ICT2_Panel-Discussion_MAT-AU-2301976
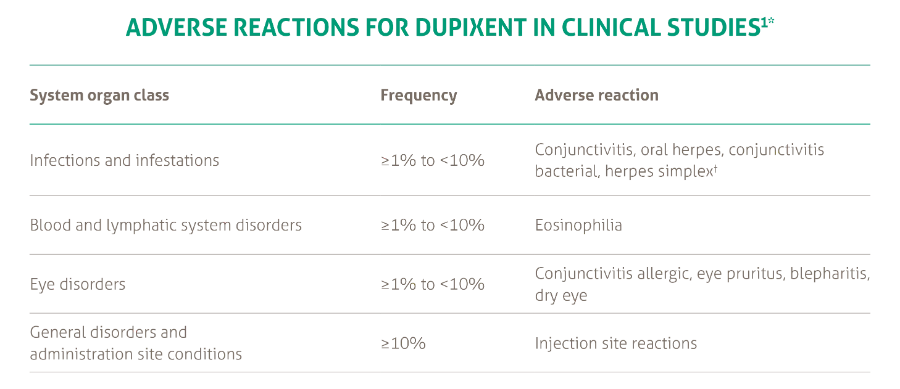
SANA7993_Safety-Page-Tables_V0.2_1_New3
Products_Dermatology_Atopic-Dermatitis_Adverse-Events-Adults_18012021