Pertussis
Discover timely medical updates and key resources on preventing and controlling pertussis – helping you stay informed and improve patient outcomes.
*Image is not an actual patient.
About pertussis
The challenges of pertussis
Pertussis, also known as whooping cough, is a highly contagious disease of the respiratory tract caused by Bordetella pertussis, a bacterium that lives in the mouth, nose, and throat. The disease is most dangerous in infants and spreads easily from person to person, mainly through droplets produced by coughing or sneezing. The first symptoms generally appear 7–10 days after infection, and include mild fever, runny nose, and cough, which in typical cases, gradually develops into a paroxysmal cough followed by whooping. In the youngest infants, the paroxysms may be followed by periods of apnoea. Pneumonia is a relatively common complication; seizures and encephalopathy occur more rarely. Untreated patients may be contagious for three weeks or more following onset of the cough. Pertussis can be prevented by immunisation.1–3
Don’t miss these key links
Signs and symptoms
Pertussis has an insidious onset. The first stage of the disease usually starts within 7-10 days and is characterised by catarrhal symptoms such as coryza, low-grade fever, and mild occasional cough that are indistinguishable from those of minor respiratory tract infections. The patient is highly contagious during this time.1,2
In the second stage i.e. paroxysmal, the cough, which is initially intermittent, becomes paroxysmal. In typical cases paroxysms terminate with inspiratory whoop and posttussive vomiting can follow. Paroxysms of cough, which may occur more at night, usually increase in frequency and severity as the illness progresses and typically persists for 1 to 6 weeks but may persist for up to 10 weeks. Exhaustion and cyanosis are other symptoms observed in this stage. The patient is most contagious up until first 2 weeks following the onset of cough. The paroxysmal cough disappears gradually in the convalescent stage which usually lasts for 7-10 days. The patient is no longer contagious at this time. After paroxysms subside, a non-paroxysmal cough can continue for 2 to 6 weeks or longer. Paroxysms may recur whenever the patient suffers any subsequent respiratory infection up to many months after initial pertussis infection.2,4
The symptoms of pertussis can be milder and the characteristic “whoop” absent in previously vaccinated children, adolescents, and adults.2
Babies and infants
In infants, the cough may be minimal or absent, and apnoea may be the only symptom. Unvaccinated or incompletely vaccinated infants younger than 12 months of age have the highest risk for severe complications and death.2 Complications in infants include pneumonia, seizures, and hypoxic encephalopathy, which may be fatal.5
Adolescents and adults
The severity of symptoms may vary in adults. Symptoms are generally less severe than babies and infants, and the typical “whoop” is less frequently seen and may be absent.4 In adults and adolescents the disease is characterised with a prolonged, persistent, nonspecific cough.2 Complications in adults can include weight loss, urinary incontinence, syncope, rib fracture due to severe coughing, anorexia, dehydration, epistaxis, hernias, and otitis media. More severe complications can include encephalopathy as a result of hypoxia from coughing or possibly from toxin, pneumothorax, rectal prolapse, subdural hematomas, and seizures.6
Diagnosis
Pertussis is usually diagnosed by the presence of clinical symptoms characteristic of the disease. Etiological diagnosis is based on recovering B. pertussis from nasopharyngeal specimens including nasopharyngeal swab or aspirate. Traditionally, bacterial culture has been considered the gold standard for laboratory confirmation because it is the only 100% specific method for identification. For ideal diagnosis using blood culture the specimen must be collected during the first 2 weeks of the disease as during this time viable bacteria are present in the nasopharynx. Any specimen collected after this duration may be less sensitive and lead to false negative results. Other tests that can be performed include polymerase chain reaction (PCR) and serology. PCR is a highly specific and rapid test. However its specificity varies, so during an outbreak it is recommended to confirm at least one case using blood culture. With PCR the specimen should ideally be collected during the first 3 weeks of illness. However, an accurate result can be achieved up to 4 weeks after which risk of false negative result increases due to rapidly decreasing amount of bacterial DNA in the nasopharynx.
Serologic tests are more useful for diagnosis in later phases of the disease with the optimum time being 2 to 8 weeks following cough onset, when the antibody titres are at their highest. These tests can also be performed using specimens collected up until 12 weeks from cough onset.7
Prevention
Pertussis can be prevented by immunization. Pertussis vaccine is only available in Australia in combination with diphtheria and tetanus, with or without other antigens such as inactivated poliomyelitis, hepatitis B and Haemophilus influenzae type b.
Bacteriology
Pertussis is caused by Bordetella pertussis, a fastidious, Gram-negative, pleomorphic bacillus.5
Epidemiology
Despite a long-standing immunisation program, pertussis remains highly prevalent in Australia and the least well controlled of all vaccine-preventable diseases with epidemics occurring every 3 to 4 years. In unvaccinated populations, these outbreaks can be very large. In vaccinated populations, outbreaks are smaller, with greatly reduced mortality and morbidity, and may continue to occur every 3 to 4 years or be more widely spaced. The maximal risk of infection and severe morbidity is before infants are old enough to be fully immunised.5 In recent years, among highly immunised communities, many cases of pertussis have occurred in adults and adolescents due to waning immunity, making them a significant reservoir of infection.5,8 Studies of infant pertussis cases indicate household contacts and carers as the source of infection, with parents identified as the source for more than 50% of cases.9 However, Australian studies have shown that in settings where notification rates in children are high, siblings are a significant source of infant infections.10 There have also been case reports documenting nosocomial infection in young infants acquired from healthcare workers.11
Treatment
Antibiotics can be used for the treatment of pertussis. Early treatment of pertussis is very important because antibiotics may mitigate clinical pertussis when given during the first 1 to 2 weeks before coughing paroxysms occur. When given later, antimicrobial drugs do not change the clinical course. Persons with pertussis are infectious from the beginning of the catarrhal stage through the third week after the onset of paroxysms or until 5 days after the start of effective antimicrobial treatment.
Featured content

Register to receive full access (Healthcare Professionals Only)
Are you a registered healthcare professional?
Register in less than a minute to access the latest updates and resources to support your practice and help deliver better outcomes for your patients.
Can’t find what you’re looking for?
Search our extensive Content Library
- World Health Organization. Pertussis. Overview. https://www.who.int/health-topics/pertussis#tab=tab_1. Accessed March 1 2024.
- Centers for Disease Control and Prevention. Pertussis (Whooping cough). Clinical Features. https://www.cdc.gov/pertussis/clinical/features.html. Accessed March 1 2024.
- Centers for Disease Control and Prevention. Pertussis (Whooping cough). Prevention. https://www.cdc.gov/pertussis/clinical/prevention.html. Accessed March 1 2024.
MAT-AU-2501407 - 1.0 - 07/2025
Waddling-Gait---Robert,-28-year-old-mild-LOPD-patient
Waddling Gait - Robert, 28-year-old mild LOPD patient
Reaching-Overhead---Robert,-28-year-old-mild-LOPD-patient
Reaching Overhead - Robert, 28-year-old mild LOPD patient
Standing-From-Sitting---Robert,-28-year-old-mild-LOPD-patient
Standing From Sitting - Robert, 28-year-old mild LOPD patient
Climbing-Stairs---Robert,-28-year-old-mild-LOPD-patient
Climbing Stairs - Robert, 28-year-old mild LOPD patient
Waddling-Gait---Karen,-18-year-old-moderate-LOPD-patient

Waddling Gait - Karen, 18-year-old moderate LOPD patient
Reaching-Overhead---Karen,-18-year-old-moderate-LOPD-patient

Reaching Overhead - Karen, 18-year-old moderate LOPD patient
Standing-From-Sitting---Karen,-18-year-old-moderate-LOPD-patient

Standing From Sitting - Karen, 18-year-old moderate LOPD patient
Climbing-Stairs---Karen,-18-year-old-moderate-LOPD-patient

Climbing Stairs - Karen, 18-year-old moderate LOPD patient
ASPIRE-ICT-1-23_Harrington_MAT-AU-2302788-1

ASPIRE-ICT-1-23_Kyle-Blakey_MAT-AU-2302789-1

Which-biologic-and-why--When-to-switch-to-another-one-

Waddling-Gait---Brian,-44-year-old-severe-LOPD-patient

Waddling Gait - Brian, 44-year-old severe LOPD patient
Reaching-Overhead---Brian,-44-year-old-severe-LOPD-patient

Reaching Overhead - Brian, 44-year-old severe LOPD patient
Standing-From-Sitting---Brian,-44-year-old-severe-LOPD-patient

Standing From Sitting - Brian, 44-year-old severe LOPD patient
Climbing-Stairs---Brian,-44-year-old-severe-LOPD-patient

Climbing Stairs - Brian, 44-year-old severe LOPD patient
RESP-ICT2_Wark_MAT-AU-2301970
.webp/jcr:content/RESP-ICT2-Wark_400X300%20(1).webp)
RESP-ICT2_Wark_MAT-AU-2301970
RESP-ICT2_Stone_MAT-AU-2301972
.webp/jcr:content/RESP-ICT2-Stone_400X300%20(1).webp)
RESP-ICT2_Stone_MAT-AU-2301972
Remission-in-rheumatology---Dr-Michelle-Tellus
.webp/jcr:content/RESP-ICT2-Tellus_400X300%20(1).webp)
Remission in rheumatology - Dr Michelle Tellus
Pavord_MAT-AU-2300571

Pavord_MAT-AU-2300571
Wark_MAT-AU-2300572

Wark_MAT-AU-2300572
Q-A-Discussion_MAT-AU-2300573

Q&A-Discussion_MAT-AU-2300573
RESP-ICT3_Tellus_MAT-AU-2302033

RESP-ICT3_Tellus_MAT-AU-2302033
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Hew_MAT-AU-2302035

RESP-ICT3_Hew_MAT-AU-2302035
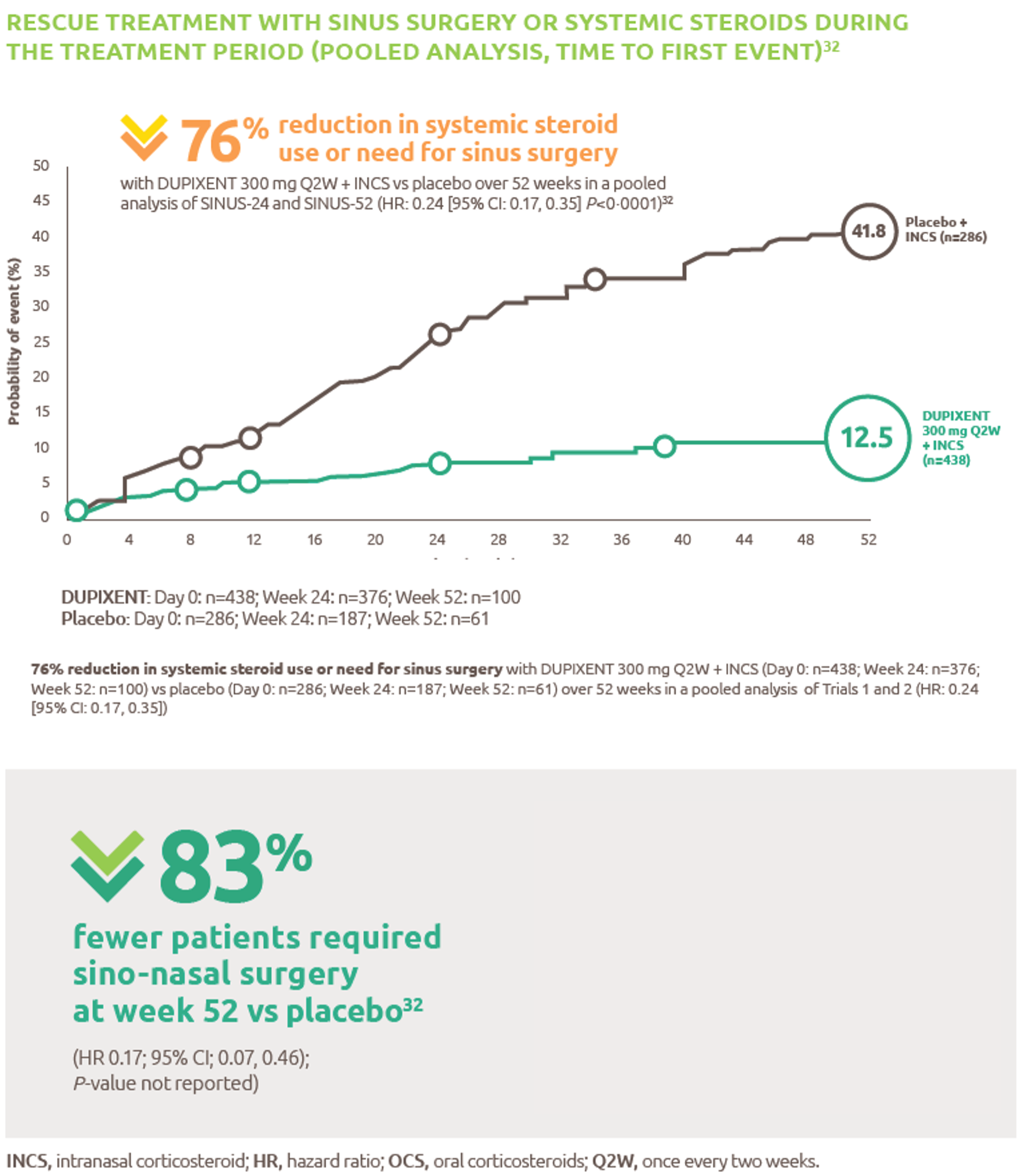
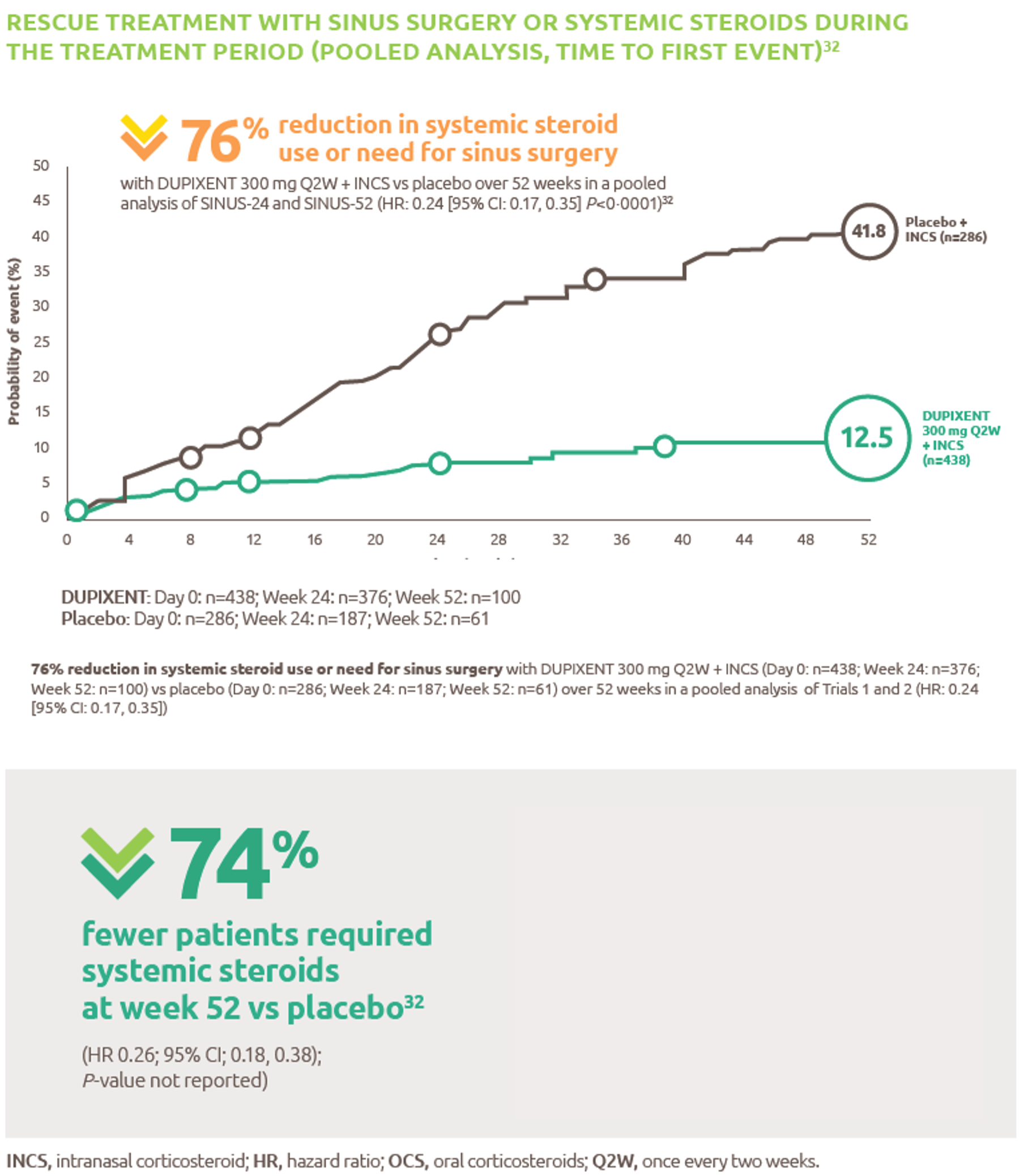
Reduced-need-for-sinus-surgery
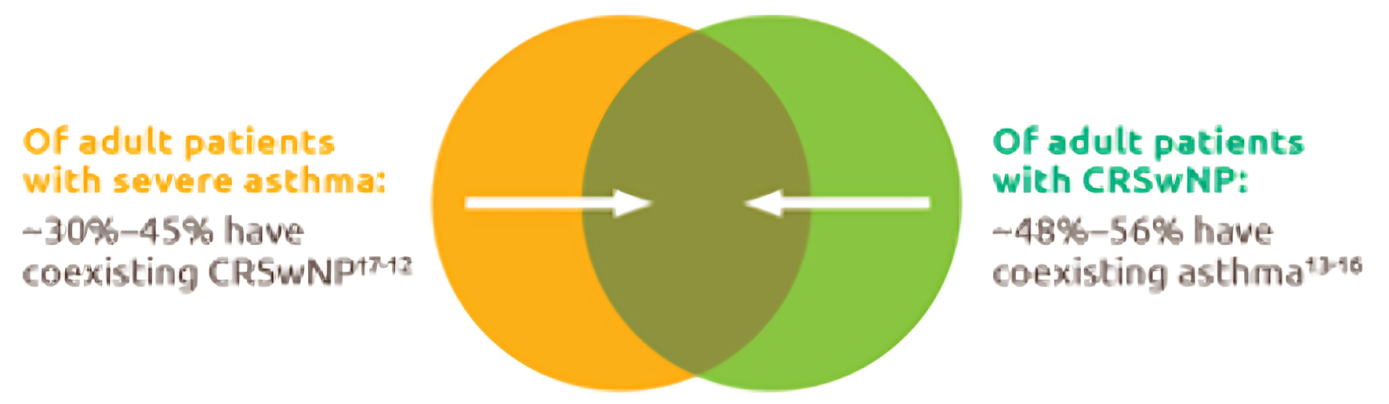
Up-to-45--of-severe-asthma-patients-have-comorbid-CRSwNP
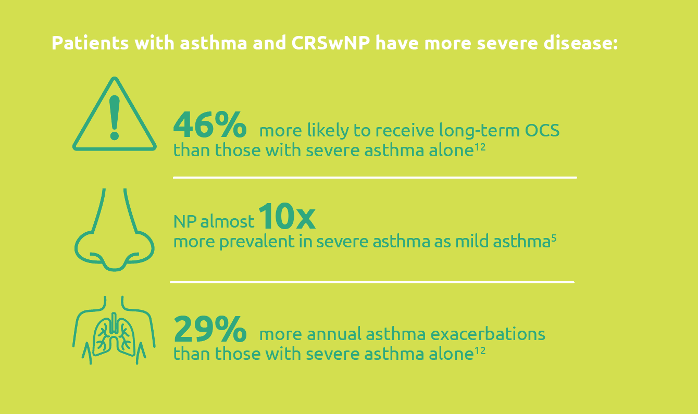
Severe-asthma-with-comorbid-CRSwNP-leads-to-more-severe-disease
.png)
Less-rescue-oral-corticosteriod-use
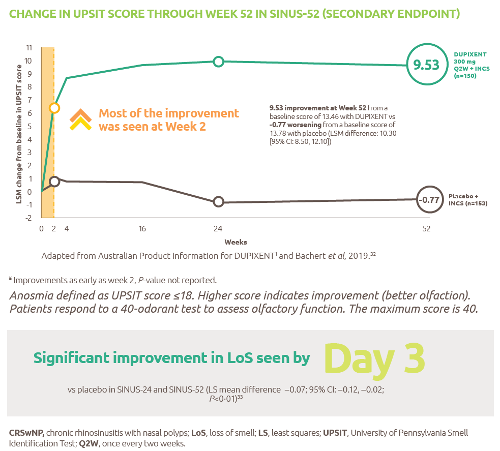
Improved-sense-of-smell
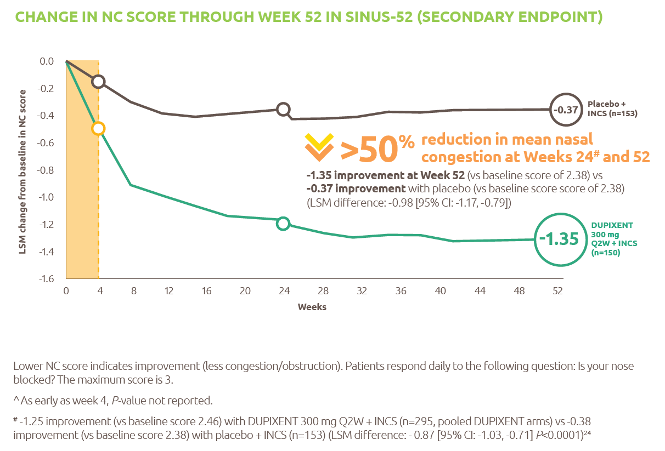
Reduced-obstruction-and-congestion
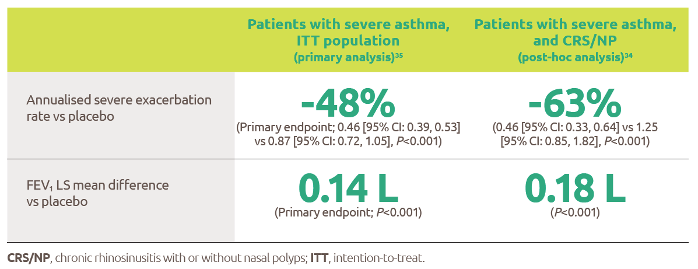
Reduced-asthma-exacerbations-and-improved-lung-function
IL-4-and-IL-13-are-key-and-central-drivers-of-type-2-inflammation

Gaucher-diagnosis-1

RESP-ICT2_Debate_MAT-AU-2301973

RESP-ICT2_Debate_MAT-AU-2301973
RESP-ICT3_Q-A_MAT-AU-2302036

RESP-ICT3_Q&A_MAT-AU-2302036
ASPIRE-ICT1-23_Q-A_MAT-AU-2302791-1

RESP-ICT2_Stone_CS_MAT-AU-2301975

RESP-ICT2_Stone_CS_MAT-AU-2301975
RESP-ICT2_Wark_CS_MAT-AU-2301974

RESP-ICT2_Wark_CS_MAT-AU-2301974
RESP-ICT2_Panel-Discussion_MAT-AU-2301976

RESP-ICT2_Panel-Discussion_MAT-AU-2301976
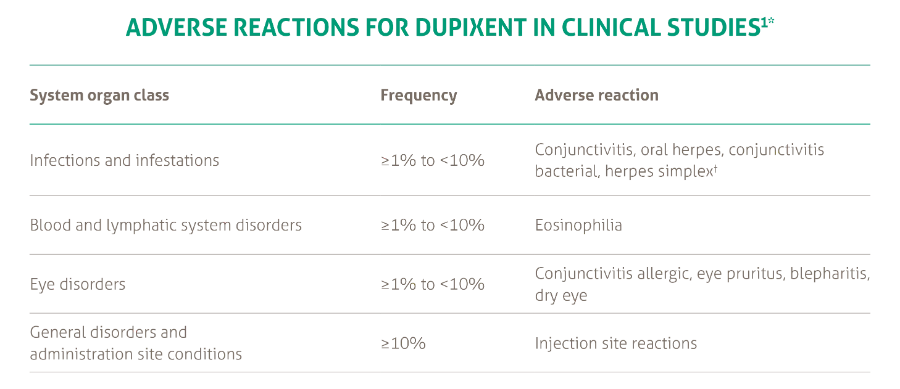
SANA7993_Safety-Page-Tables_V0.2_1_New3
Products_Dermatology_Atopic-Dermatitis_Adverse-Events-Adults_18012021