Tetanus
Discover timely medical updates and key resources on preventing and controlling tetanus – helping you stay informed and improve patient outcomes.
*Image is not an actual patient.
About tetanus
The challenges of tetanus
Tetanus is a non-communicable disease contracted through exposure to the spores of the bacterium, Clostridium tetani that exists worldwide in soil and in animal intestinal tracts, and as such can contaminate many surfaces and substances. People of all ages can get tetanus1.The spores develop into bacteria in anaerobic environment of contaminated wound and produce neurotoxin which interferes with release of neurotransmitters, blocking inhibitor impulses leading to unopposed muscle contraction and spasm. Seizures may occur, and the autonomic nervous system may also be affected1,2. Tetanus can be prevented through immunization with tetanus-toxoid-containing vaccines1.
Don’t miss these key links
Signs and symptoms
The incubation period ranges from 3 to 21 days. In general, the further the injury site is from the central nervous system, the longer the incubation period. A shorter incubation period is associated with more severe disease, complications, and a higher chance of death.
On the basis of clinical manifestations, three different forms of tetanus have been described: generalized, localized, and cephalic.
Generalized tetanus is the most common form, occurring in >80% of cases. The most common initial sign is spasm of the muscles of the jaw known as trismus or lockjaw. This may be followed by painful spasms in other muscle groups in the neck, trunk, and extremities and by generalized, seizure-like activity or convulsions in severe cases. Spasm of the glottis may cause sudden death. In neonatal tetanus, generalized spasms are commonly preceded by the inability to suck or breastfeed and excessive crying. Case-fatality rates vary from 10% to 70% depending on treatment, age and general health of the patient.
Localized tetanus is uncommon; it is characterized by sustained contraction of the muscles in the same area as the injury site. Case-fatality rates for localized tetanus are <1%. Although localized tetanus often occurs in people with partial immunity and is usually mild, progression to generalized tetanus can occur.
The rarest form, cephalic tetanus, is associated with lesions of the head or face and has been described in association with otitis media. The incubation period is short, usually 1 to 2 days and a case-fatality rate of 15–30%. Unlike generalized and localized tetanus, cephalic tetanus results in flaccid cranial nerve palsies rather than spasm. Spasm of the jaw muscles may also be present. Like localized tetanus, cephalic tetanus can progress to the generalized form 2,3.
Diagnosis
The diagnosis of tetanus is primarily based on clinical features and does not depend on laboratory confirmation. The WHO definition of a confirmed neonatal tetanus case is an illness occurring in an infant who has the normal ability to suck and cry in the first 2 days of life, but loses this ability between days 3 and 28 of life and becomes rigid or has spasms. The WHO definition of adult tetanus requires at least one of the following signs: trismus or risus sardonicus; or painful muscular contractions. Although this definition requires a history of injury or wound, tetanus may also occur in patients who are unable to recall a specific wound or injury.
A clinical test, the “spatula test”, may be performed, in which tetanus is diagnosed by reflex spasm of the jaw in response to touching the posterior wall of the pharynx with a soft instrument. This test has high specificity (100%) and sensitivity (94%) 3
Prevention
Tetanus can be prevented through immunization with tetanus-toxoid (TT) containing vaccines. Tetanus toxoid is available in Australia only in combination with diphtheria, with or without other antigens such as pertussis, inactivated poliomyelitis, hepatitis B and Haemophilus influenzae type b.
Bacteriology
Tetanus is caused by Clostridium tetani, a motile, non-capsulated, Gram-positive rod that forms endospores. Spores of the bacillus are commonly found in manured soil and can enter wounds. Once in a wound site, the bacillus can grow anaerobically. C. tetani produces a potent protein toxin, which has two components, tetanospasmin (a neurotoxin) and tetanolysin (a haemolysin)2.
Epidemiology
In Australia, tetanus is rare, occurring primarily in adults who have never been vaccinated, or who have not received a recent tetanus booster. Fourteen cases of tetanus were notified in Australia between 2016 and 2018; however 52 tetanus-related hospitalisations were reported during the same period, suggesting that the disease is underreported in Australia.
The Australian National Serosurvey has shown progressively lower levels of tetanus antibody in older age groups, particularly in women4. Although the tetanus organism is universally present in the environment, and the vaccine only provides individual level of protection against the toxin, tetanus vaccination programs have had a significant impact on disease control in Australia.
Treatment
Tetanus is a medical emergency requiring hospitalization, immediate treatment with human tetanus immunoglobulin, agents to control muscle spasm, appropriate wound care, antibiotics, and a tetanus toxoid booster.
A patent airway should be maintained and, depending on the severity of disease, endotracheal intubation or tracheostomy and mechanically assisted respiration may be lifesaving. Sedation and muscle relaxant drugs should be used as indicated to control muscle spasms. Agents to control autonomic nervous system instability may be required. Active immunization may be initiated concurrently with treatment2.
Featured content

Register to receive full access (Healthcare Professionals Only)
Are you a registered healthcare professional?
Register in less than a minute to access the latest updates and resources to support your practice and help deliver better outcomes for your patients.
Can’t find what you’re looking for?
Search our extensive Content Library
- Tetanus. Immunization, Vaccines and Biologicals. World Health Organization. http://www.who.int/immunization/diseases/tetanus/en/. Accessed 07/2025.
- Australian Immunisation Handbook 10th edition. Australian Govt. Department of health. https://immunisationhandbook.health.gov.au/vaccine-preventable-diseases/tetanus. Accessed 07/2025.
- Tetanus vaccines: World Health Organization (WHO) position paper. WHO. Weekly epidemiological record No. 6. 2017; 92: 53–76.
- Gidding HF, Backhouse JL, Gilbert GL, Burgess MA. Immunity to diphtheria and tetanus in Australia: a national serosurvey. Med J Aust. 2005; 183 (6): 301-304..
MAT-AU-2501354 - 1.0 - 03/2024
Waddling-Gait---Robert,-28-year-old-mild-LOPD-patient
Waddling Gait - Robert, 28-year-old mild LOPD patient
Reaching-Overhead---Robert,-28-year-old-mild-LOPD-patient
Reaching Overhead - Robert, 28-year-old mild LOPD patient
Standing-From-Sitting---Robert,-28-year-old-mild-LOPD-patient
Standing From Sitting - Robert, 28-year-old mild LOPD patient
Climbing-Stairs---Robert,-28-year-old-mild-LOPD-patient
Climbing Stairs - Robert, 28-year-old mild LOPD patient
Waddling-Gait---Karen,-18-year-old-moderate-LOPD-patient

Waddling Gait - Karen, 18-year-old moderate LOPD patient
Reaching-Overhead---Karen,-18-year-old-moderate-LOPD-patient

Reaching Overhead - Karen, 18-year-old moderate LOPD patient
Standing-From-Sitting---Karen,-18-year-old-moderate-LOPD-patient

Standing From Sitting - Karen, 18-year-old moderate LOPD patient
Climbing-Stairs---Karen,-18-year-old-moderate-LOPD-patient

Climbing Stairs - Karen, 18-year-old moderate LOPD patient
ASPIRE-ICT-1-23_Harrington_MAT-AU-2302788-1

ASPIRE-ICT-1-23_Kyle-Blakey_MAT-AU-2302789-1

Which-biologic-and-why--When-to-switch-to-another-one-

Waddling-Gait---Brian,-44-year-old-severe-LOPD-patient

Waddling Gait - Brian, 44-year-old severe LOPD patient
Reaching-Overhead---Brian,-44-year-old-severe-LOPD-patient

Reaching Overhead - Brian, 44-year-old severe LOPD patient
Standing-From-Sitting---Brian,-44-year-old-severe-LOPD-patient

Standing From Sitting - Brian, 44-year-old severe LOPD patient
Climbing-Stairs---Brian,-44-year-old-severe-LOPD-patient

Climbing Stairs - Brian, 44-year-old severe LOPD patient
RESP-ICT2_Wark_MAT-AU-2301970
.webp/jcr:content/RESP-ICT2-Wark_400X300%20(1).webp)
RESP-ICT2_Wark_MAT-AU-2301970
RESP-ICT2_Stone_MAT-AU-2301972
.webp/jcr:content/RESP-ICT2-Stone_400X300%20(1).webp)
RESP-ICT2_Stone_MAT-AU-2301972
Remission-in-rheumatology---Dr-Michelle-Tellus
.webp/jcr:content/RESP-ICT2-Tellus_400X300%20(1).webp)
Remission in rheumatology - Dr Michelle Tellus
Pavord_MAT-AU-2300571

Pavord_MAT-AU-2300571
Wark_MAT-AU-2300572

Wark_MAT-AU-2300572
Q-A-Discussion_MAT-AU-2300573

Q&A-Discussion_MAT-AU-2300573
RESP-ICT3_Tellus_MAT-AU-2302033

RESP-ICT3_Tellus_MAT-AU-2302033
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Hew_MAT-AU-2302035

RESP-ICT3_Hew_MAT-AU-2302035
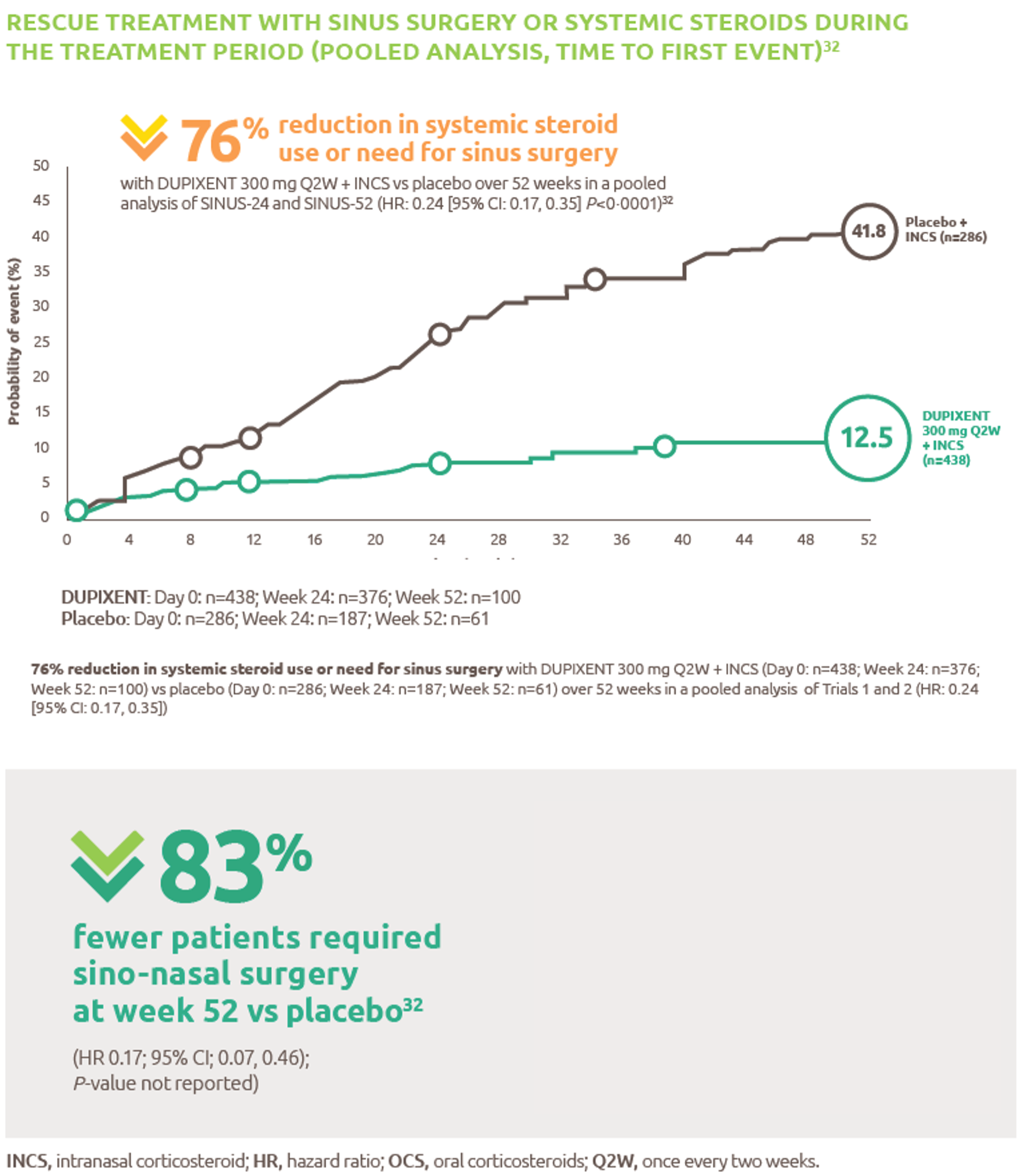
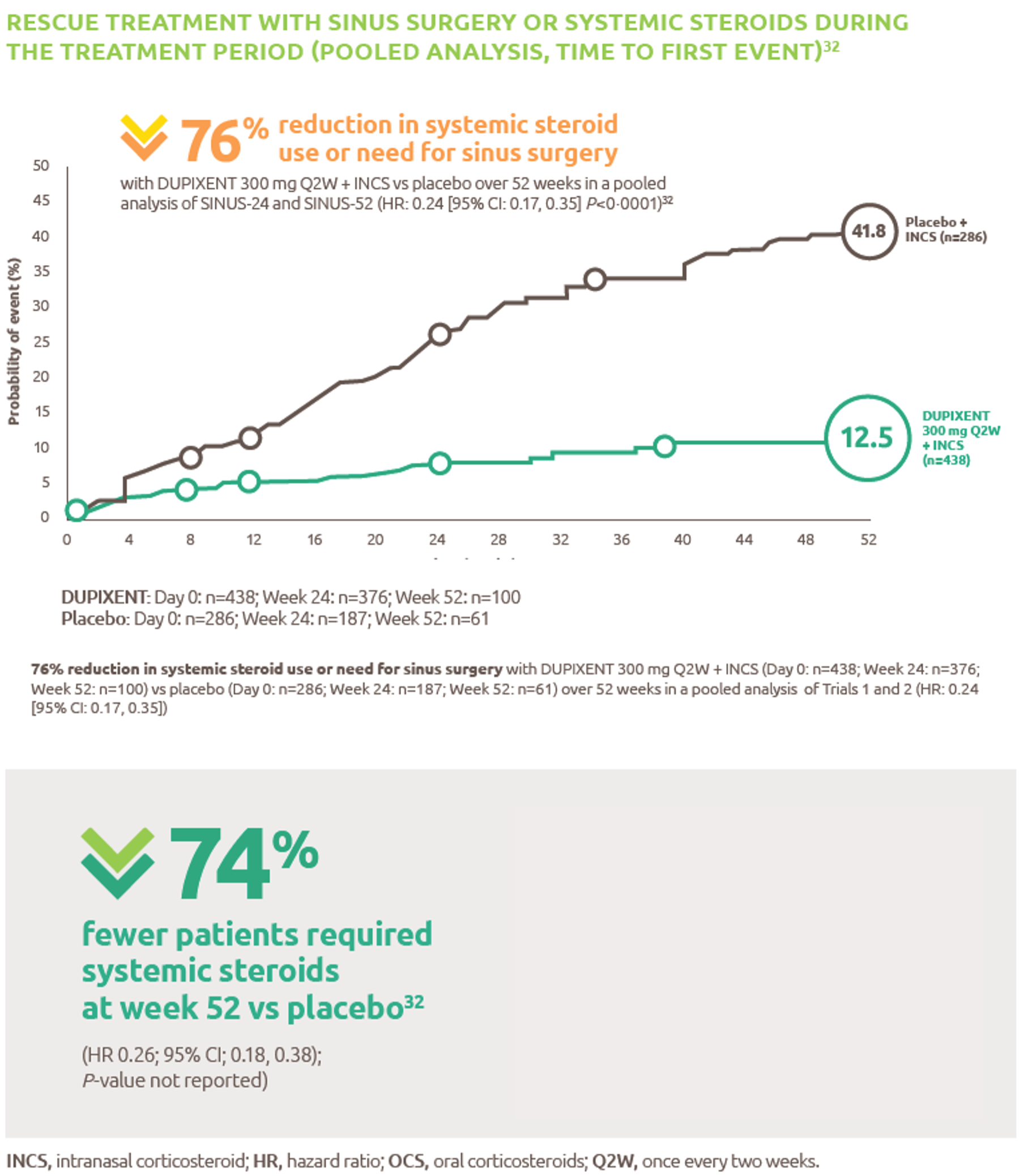
Reduced-need-for-sinus-surgery
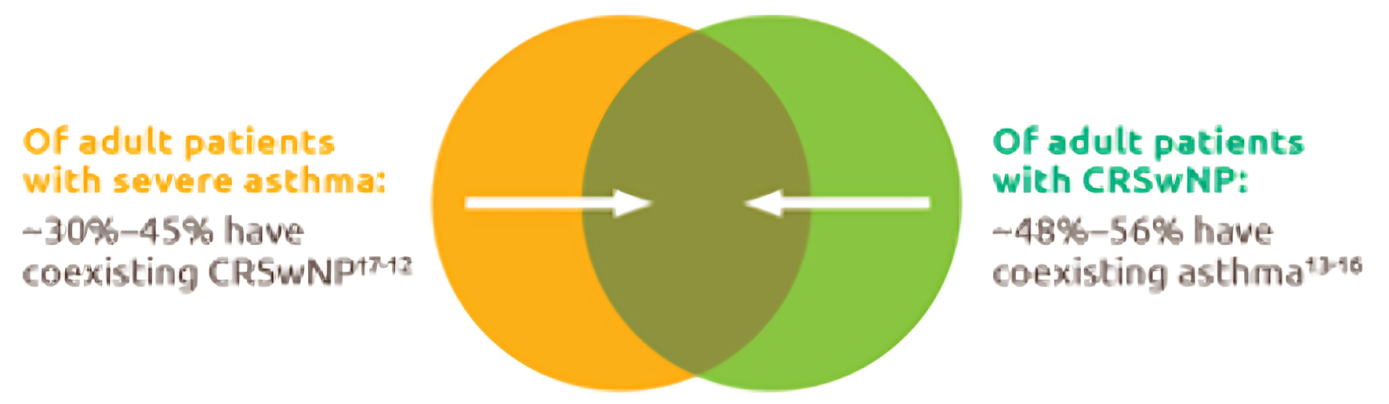
Up-to-45--of-severe-asthma-patients-have-comorbid-CRSwNP
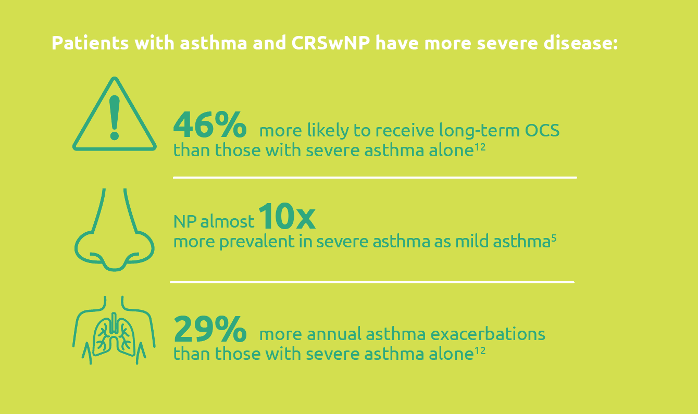
Severe-asthma-with-comorbid-CRSwNP-leads-to-more-severe-disease
.png)
Less-rescue-oral-corticosteriod-use
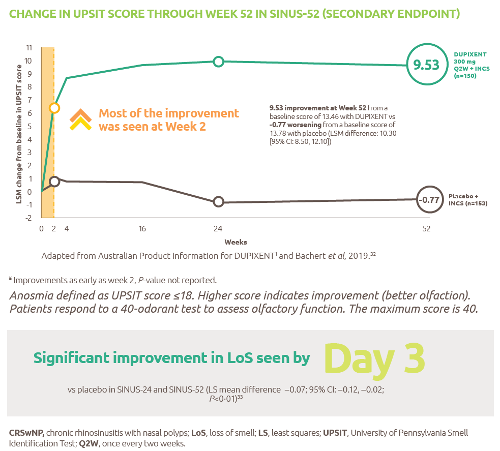
Improved-sense-of-smell
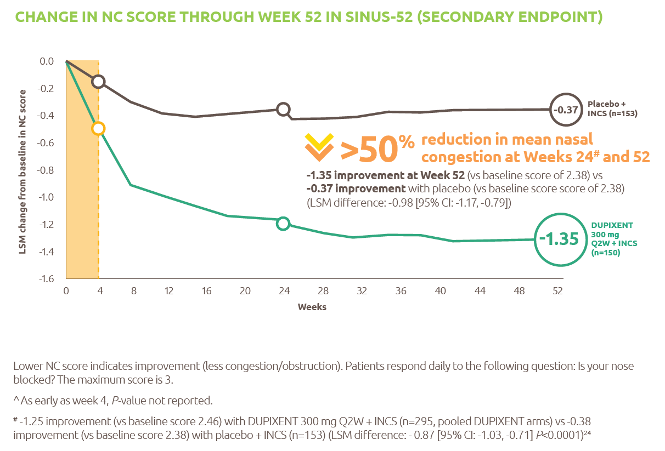
Reduced-obstruction-and-congestion
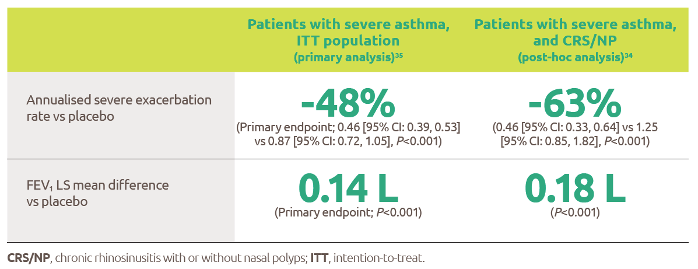
Reduced-asthma-exacerbations-and-improved-lung-function
IL-4-and-IL-13-are-key-and-central-drivers-of-type-2-inflammation

Gaucher-diagnosis-1

RESP-ICT2_Debate_MAT-AU-2301973

RESP-ICT2_Debate_MAT-AU-2301973
RESP-ICT3_Q-A_MAT-AU-2302036

RESP-ICT3_Q&A_MAT-AU-2302036
ASPIRE-ICT1-23_Q-A_MAT-AU-2302791-1

RESP-ICT2_Stone_CS_MAT-AU-2301975

RESP-ICT2_Stone_CS_MAT-AU-2301975
RESP-ICT2_Wark_CS_MAT-AU-2301974

RESP-ICT2_Wark_CS_MAT-AU-2301974
RESP-ICT2_Panel-Discussion_MAT-AU-2301976

RESP-ICT2_Panel-Discussion_MAT-AU-2301976
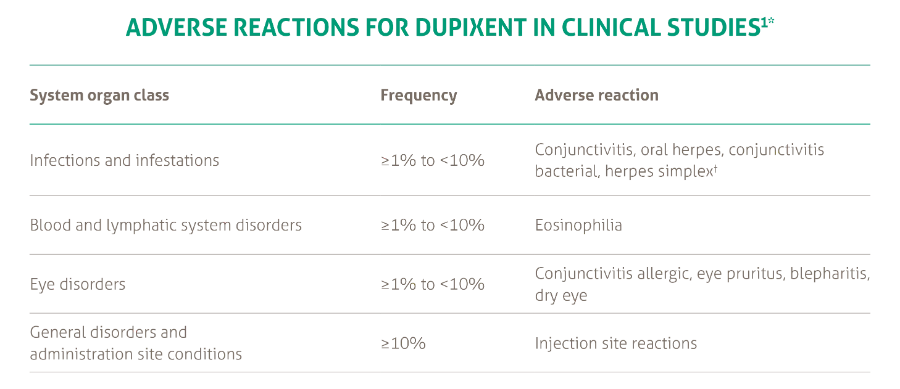
SANA7993_Safety-Page-Tables_V0.2_1_New3
Products_Dermatology_Atopic-Dermatitis_Adverse-Events-Adults_18012021