Meningococcal Disease
Discover timely medical updates and key resources on preventing and controlling meningococcal disease – helping you stay informed and improve patient outcomes.
*Image is not an actual patient.
About meningococcal disease
The challenges of meningococcal disease
Meningococcal disease is caused by the Gram-negative bacterium, Neisseria meningitidis, commonly known as meningococcus.1 Transmission occurs by close person-to-person contact involving saliva or nasopharyngeal secretions (eg. kissing, drinking from the same cup) and through respiratory droplets.1 Human beings are the only reservoir of Neisseria meningitidis and people can carry N.meningitidis without developing any disease andpeople (especially adolescents) can carry N.meningitidis and transmit to others without knowing because carnage of the bacterium does not cause any symptoms. Prevalence of carriage is higher when groups of people occupy small areas of living space.1 Living in crowded conditions increase risk of carry the bacteruim. (eg students, military recruits) and adolescents and young adults have the highest carriage rates.2
Supporting meningococcal disease management through information
Effective management and prevention of meningococcal disease involves a comprehensive understanding of the condition. For healthcare professionals, staying informed about the disease and evolving epidemiology and science is crucial for providing care.
To foster a broader understanding of meningococcal disease, this page offers a range of selected materials and information.
Understanding meningococcal disease research and care
Providing robust protection against meningococcal disease requires a strong commitment to understand, treat, and prevent the disease. Here are broad areas of focus in meningococcal disease research:
- Performing global strain surveillance to track serogroup distribution
- Providing immediate antibiotic therapy upon suspicion
- Deploying conjugate vaccines in mass campaigns and routine immunization
Don’t miss these key links
Signs and symptoms
N.meningitidis can cause serious condition called invasive meningococcal disease (IMD), which usually presents as meningitis and septicaemia. Symptoms may be non-specific and can include a sudden onset of fever, headache, nausea, vomiting, sensitivity to light, a stiff neck leading to lack of consciousness and in serious cases, may lead to death.1
Meningococcal infections can progress rapidly to serious disease or death in previously healthy people. The overall mortality risk for IMD is high (5–10%), even if the person receives appropriate antibiotic therapy.1
The average incubation period is 3-4 days but can range between 1 and 10 days.2
Permanent sequelae may occur in up to 30% of children and adolescents who survive disease, and can include limb deformity, skin scaring, deafness and neurologic deficits.1
Diagnosis
Meningococcal disease can be difficult to diagnose because initial signs and symptoms are often similar to those of other common diseases.3,6 Initial diagnosis of meningitis can be made by clinical examination and testing of blood and/or cerebrospinal fluid. The diagnosis is confirmed by growing the bacteria from specimens of cerebrospinal fluid or blood, by rapid diagnostic tests or by polymerase chain reaction (PCR). The identification of the serogroups and susceptibility testing to antibiotics are important for providing optimal treatment and determining control measures at population level.4,6
Prevention
Vaccination There are several meningococcal vaccines available in Australia designed to protect against (A, B, C, W and/or Y). However, there is no single vaccine that offers protection against all meningococcal serogroups.
Please refer to the Australian Immunisation Handbook as well as your local State/Territory guidelines for further information about current recommendations.
Close Contacts In some cases, vaccination or clearance antibiotics may be indicated for close contacts of people diagnosed with meningococcal disease. The relevant state or territory public health authority should be contacted as soon as possible for guidance.2
Bacteriology
There are 13 known meningococcal serogroups, distinguished by differences in surface polysaccharides of the bacterium’s outer membrane capsule. Globally, serogroups A, B, C, W and Y most commonly cause disease.1
Epidemiology
Meningococcal disease can occur sporadically or in. In Australia, cases of meningococcal disease mostly occur in winter or early spring. Most meningococcal disease occurs in young children aged <2 years and in older adolescents and young adults aged 15–24 years.2
As recorded by the NNDSS, notifications of IMD in Australia peaked in 2002 at 3.5 cases per 100,000 persons, with the majority of disease at that time caused by MenB and MenC. In 2003 the introduction of the conjugate serogroup C meningococcal vaccine to the National Immunisation Program was followed by significant and sustained reduction of both the number of serogroup C IMD, and the overall notifications to 0.6 cases per 100,000 in 2013.5
By 2017 the IMD notification rates had increased again, to 1.5 cases per 100,000, corresponding with increase in predominantly MenW and Meny. Targeted MenACWY immunisation programmes were implemented and followed by a change in the NIP in 2018, substituting monovalent MenC vaccine with the quadrivalent MenACWY vaccine. IMD notifications started to decline to 1.1 per 100,000 in 2018, and 0.8 per 100,000 in 2019 In 2020, there were 0.4 cases per 100,000 recorded and a continued reduction was recorded in 2021, to 0.3 cases per 100,000. This reduction in disease rate was beyond the expected vaccine impact and was likely attributable to the impact of public health measures implemented in response to the SARS-CoV-2 pandemic. In 2022, with the gradual easing of infection control containment measures, IMD notifications rose to 0.5 cases per 100,000 persons per year 5
In 2022, there were 127 IMD cases notified to the NNDSS, of which 121 were laboratory confirmed. Laboratory data were available to the AMSP for all 121 laboratory-confirmed IMD cases. In 2022, an increase in IMD notifications was seen across all jurisdictions, particularly in New South Wales, Queensland and Western Australia where notification numbers doubled from those reported in 2021. In 2022, the peak incidence of IMD occurred in winter through early spring.5
Treatment
Meningococcal disease can rapidly progress to death and should always be viewed as a medical emergency. Prompt diagnosis and medical treatment of suspected cases of meningococcal disease are critical.1 Admission to a hospital is necessary and appropriate antibiotic treatment must be started as soon as possible.2
The relevant state or territory public health authority should be contacted as soon as possible for guidance on determining the risk of disease, and the need for vaccination and clearance antibiotics for close contacts.2
Featured content

Register to receive full access (Healthcare Professionals Only)
Are you a registered healthcare professional?
Register in less than a minute to access the latest updates and resources to support your practice and help deliver better outcomes for your patients.
Can’t find what you’re looking for?
Search our extensive Content Library
- Australian Immunisation Handbook. Meningococcal Disease. Aust. Govt. Dept of Health. https://immunisationhandbook.health.gov.au/vaccine-preventable-diseases/meningococcal-disease Accessed June 2024
- Meningococcal Vaccines for Australians Fact Sheet. NCIRS https://www.ncirs.org.au/ncirs-fact-sheets-faqs/meningococcal-vaccines-australians Accessed June 2024
- Aust Govt. Dept of Health. https://www.health.gov.au/diseases/meningococcal-disease-invasive Meningococcal Disease Accessed June 2024
- World Health Organisation. Meningitis Fact Sheet. https://www.who.int/news-room/fact-sheets/detail/meningitis Accessed June 2024
- Australian Meningococcal Surveillance Program Annual Report, 2022. Communicable Disease Intelligence www1.health.gov.au/internet/main/publishing.nsf/Content/8FA6078276359430CA257BF0001A4C42/$File/australian_meningococcal_surveillance_programme_annual_report_2022.pdf Accessed June 2024
- Centres for Disease Control and Prevention. Meningococcal Disease. https://www.cdc.gov/meningococcal/about/diagnosis-treatment.html Accessed June 2024
MAT-AU-2102129 - 2.0 - 06/2024
Waddling-Gait---Robert,-28-year-old-mild-LOPD-patient
Waddling Gait - Robert, 28-year-old mild LOPD patient
Reaching-Overhead---Robert,-28-year-old-mild-LOPD-patient
Reaching Overhead - Robert, 28-year-old mild LOPD patient
Standing-From-Sitting---Robert,-28-year-old-mild-LOPD-patient
Standing From Sitting - Robert, 28-year-old mild LOPD patient
Climbing-Stairs---Robert,-28-year-old-mild-LOPD-patient
Climbing Stairs - Robert, 28-year-old mild LOPD patient
Waddling-Gait---Karen,-18-year-old-moderate-LOPD-patient

Waddling Gait - Karen, 18-year-old moderate LOPD patient
Reaching-Overhead---Karen,-18-year-old-moderate-LOPD-patient

Reaching Overhead - Karen, 18-year-old moderate LOPD patient
Standing-From-Sitting---Karen,-18-year-old-moderate-LOPD-patient

Standing From Sitting - Karen, 18-year-old moderate LOPD patient
Climbing-Stairs---Karen,-18-year-old-moderate-LOPD-patient

Climbing Stairs - Karen, 18-year-old moderate LOPD patient
ASPIRE-ICT-1-23_Harrington_MAT-AU-2302788-1

ASPIRE-ICT-1-23_Kyle-Blakey_MAT-AU-2302789-1

Which-biologic-and-why--When-to-switch-to-another-one-

Waddling-Gait---Brian,-44-year-old-severe-LOPD-patient

Waddling Gait - Brian, 44-year-old severe LOPD patient
Reaching-Overhead---Brian,-44-year-old-severe-LOPD-patient

Reaching Overhead - Brian, 44-year-old severe LOPD patient
Standing-From-Sitting---Brian,-44-year-old-severe-LOPD-patient

Standing From Sitting - Brian, 44-year-old severe LOPD patient
Climbing-Stairs---Brian,-44-year-old-severe-LOPD-patient

Climbing Stairs - Brian, 44-year-old severe LOPD patient
RESP-ICT2_Wark_MAT-AU-2301970
.webp/jcr:content/RESP-ICT2-Wark_400X300%20(1).webp)
RESP-ICT2_Wark_MAT-AU-2301970
RESP-ICT2_Stone_MAT-AU-2301972
.webp/jcr:content/RESP-ICT2-Stone_400X300%20(1).webp)
RESP-ICT2_Stone_MAT-AU-2301972
Remission-in-rheumatology---Dr-Michelle-Tellus
.webp/jcr:content/RESP-ICT2-Tellus_400X300%20(1).webp)
Remission in rheumatology - Dr Michelle Tellus
Pavord_MAT-AU-2300571

Pavord_MAT-AU-2300571
Wark_MAT-AU-2300572

Wark_MAT-AU-2300572
Q-A-Discussion_MAT-AU-2300573

Q&A-Discussion_MAT-AU-2300573
RESP-ICT3_Tellus_MAT-AU-2302033

RESP-ICT3_Tellus_MAT-AU-2302033
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Lee_MAT-AU-2302034
RESP-ICT3_Hew_MAT-AU-2302035

RESP-ICT3_Hew_MAT-AU-2302035
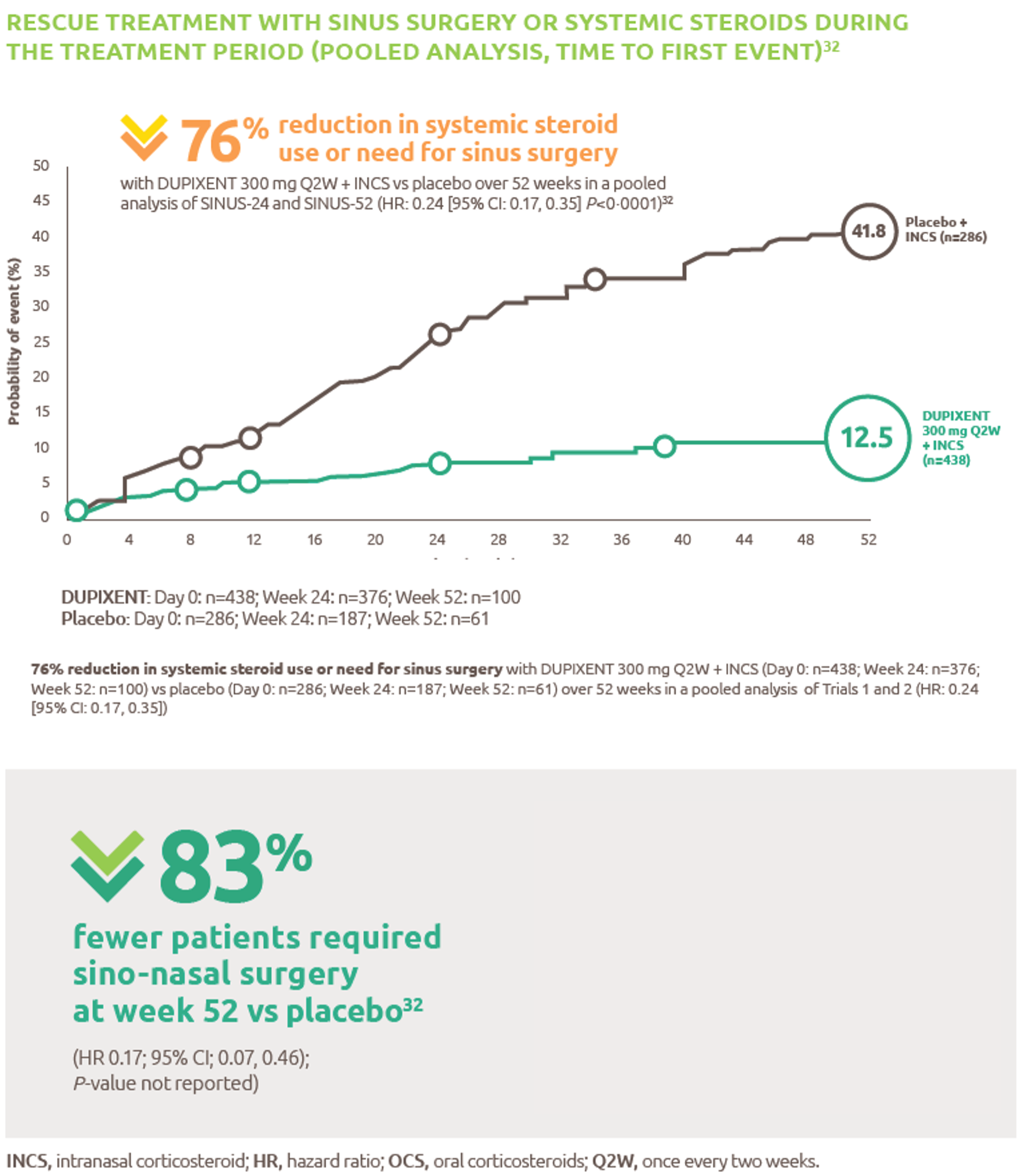
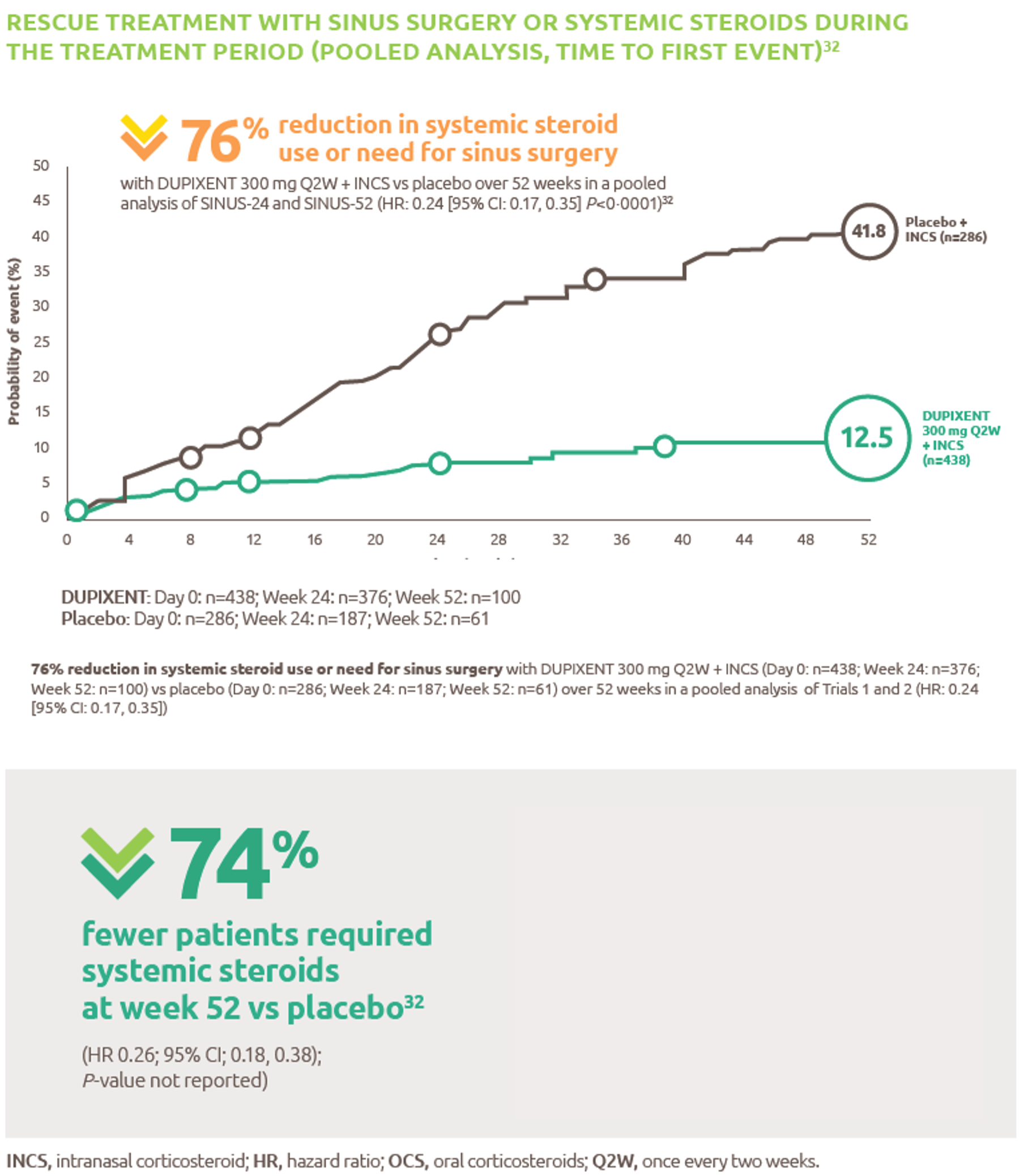
Reduced-need-for-sinus-surgery
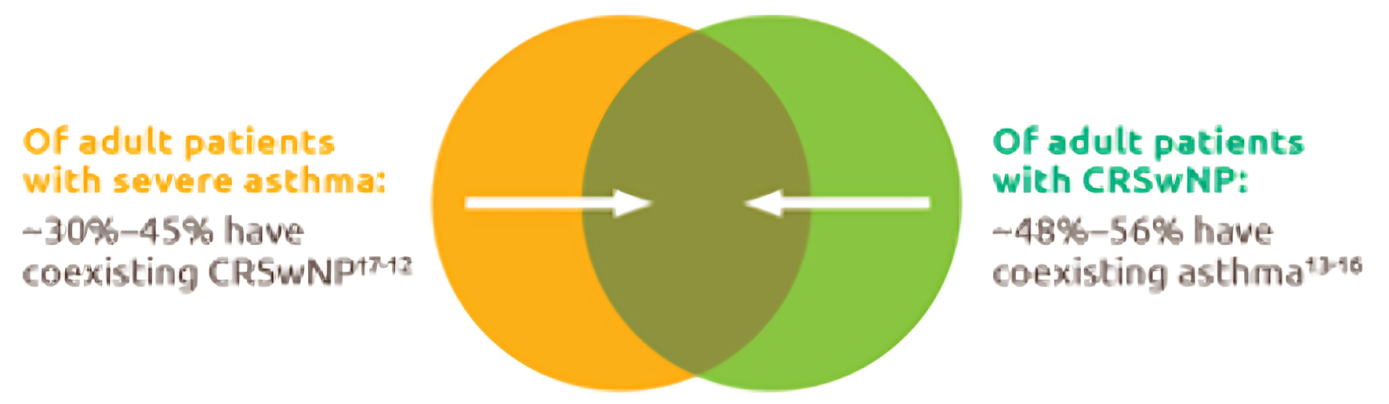
Up-to-45--of-severe-asthma-patients-have-comorbid-CRSwNP
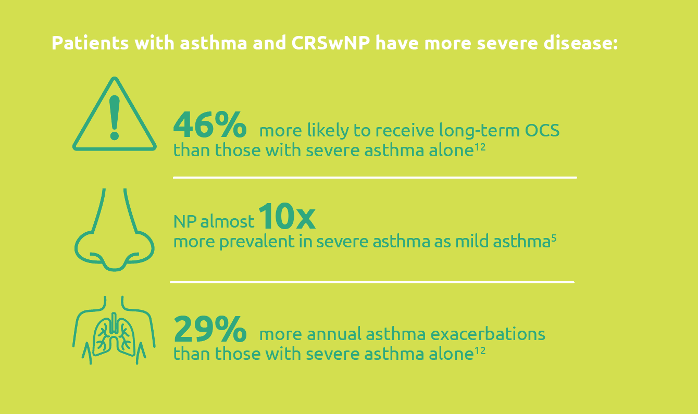
Severe-asthma-with-comorbid-CRSwNP-leads-to-more-severe-disease
.png)
Less-rescue-oral-corticosteriod-use
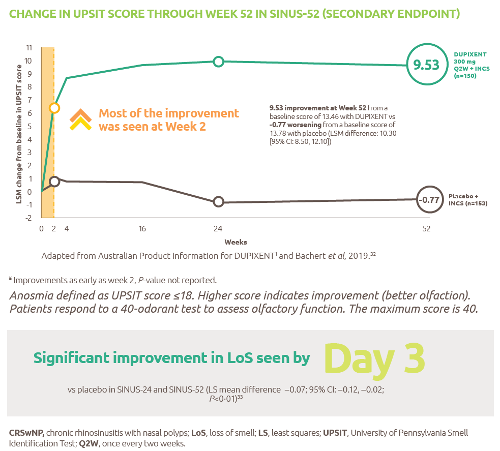
Improved-sense-of-smell
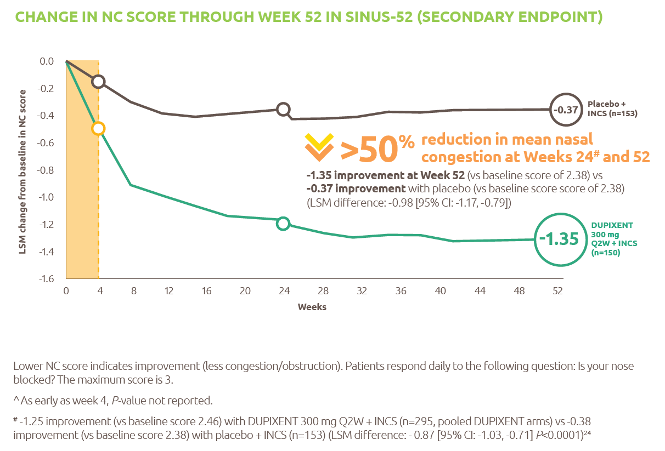
Reduced-obstruction-and-congestion
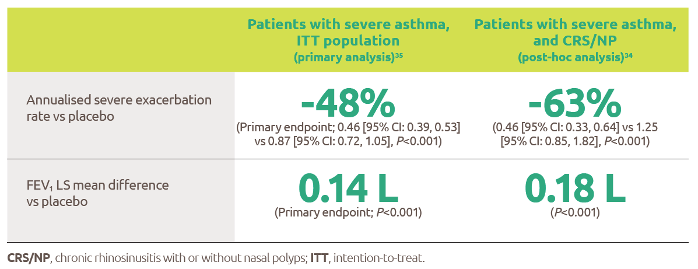
Reduced-asthma-exacerbations-and-improved-lung-function
IL-4-and-IL-13-are-key-and-central-drivers-of-type-2-inflammation

Gaucher-diagnosis-1

RESP-ICT2_Debate_MAT-AU-2301973

RESP-ICT2_Debate_MAT-AU-2301973
RESP-ICT3_Q-A_MAT-AU-2302036

RESP-ICT3_Q&A_MAT-AU-2302036
ASPIRE-ICT1-23_Q-A_MAT-AU-2302791-1

RESP-ICT2_Stone_CS_MAT-AU-2301975

RESP-ICT2_Stone_CS_MAT-AU-2301975
RESP-ICT2_Wark_CS_MAT-AU-2301974

RESP-ICT2_Wark_CS_MAT-AU-2301974
RESP-ICT2_Panel-Discussion_MAT-AU-2301976

RESP-ICT2_Panel-Discussion_MAT-AU-2301976
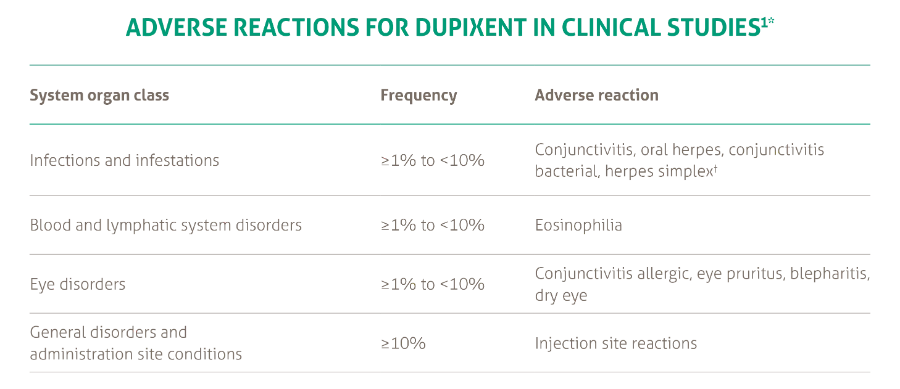
SANA7993_Safety-Page-Tables_V0.2_1_New3
Products_Dermatology_Atopic-Dermatitis_Adverse-Events-Adults_18012021