Cycle of Recurrence: A Challenge in CRSwNP Patients

Chronic rhinosinusitis with nasal polyps (CRSwNP) is a type 2 inflammatory disease associated with frequent recurrence despite effective treatments.1–5
Understanding the role of type 2 inflammation, contributing factors, and treatment strategies, including biologics, can improve management and prevent relapse, potentially offering better outcomes for CRSwNP patients.1–7
Overview of CRSwNP |
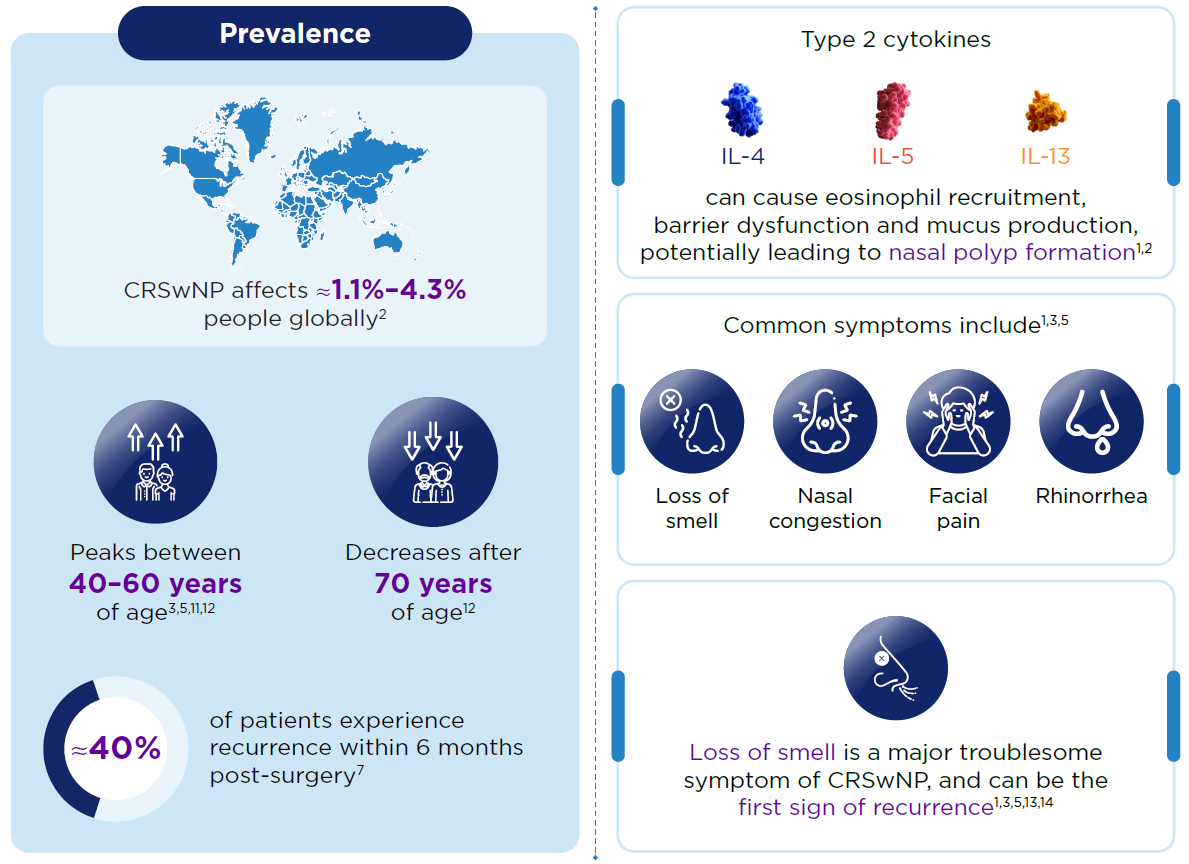
- CRSwNP is predominantly driven by type 2 inflammation.1,2
- Despite standard of care (SoC) treatments such as intranasal corticosteroids (INCS), systemic corticosteroids (SCS), and endoscopic sinus surgery (ESS), recurrence of nasal polyps is common.2,5–8
- Common symptoms include loss of smell and nasal congestion, significantly impacting patients' quality of life.1,3
- Persistent inflammation can contribute to the recurrence of nasal polyps, even after surgical intervention.4
- EPOS 2020 and ICAR 2021 guidelines recommend biologics for CRSwNP patients.3,9
Type 2 inflammation plays a central role in CRSwNP, affecting up to 87% patients1,10 |
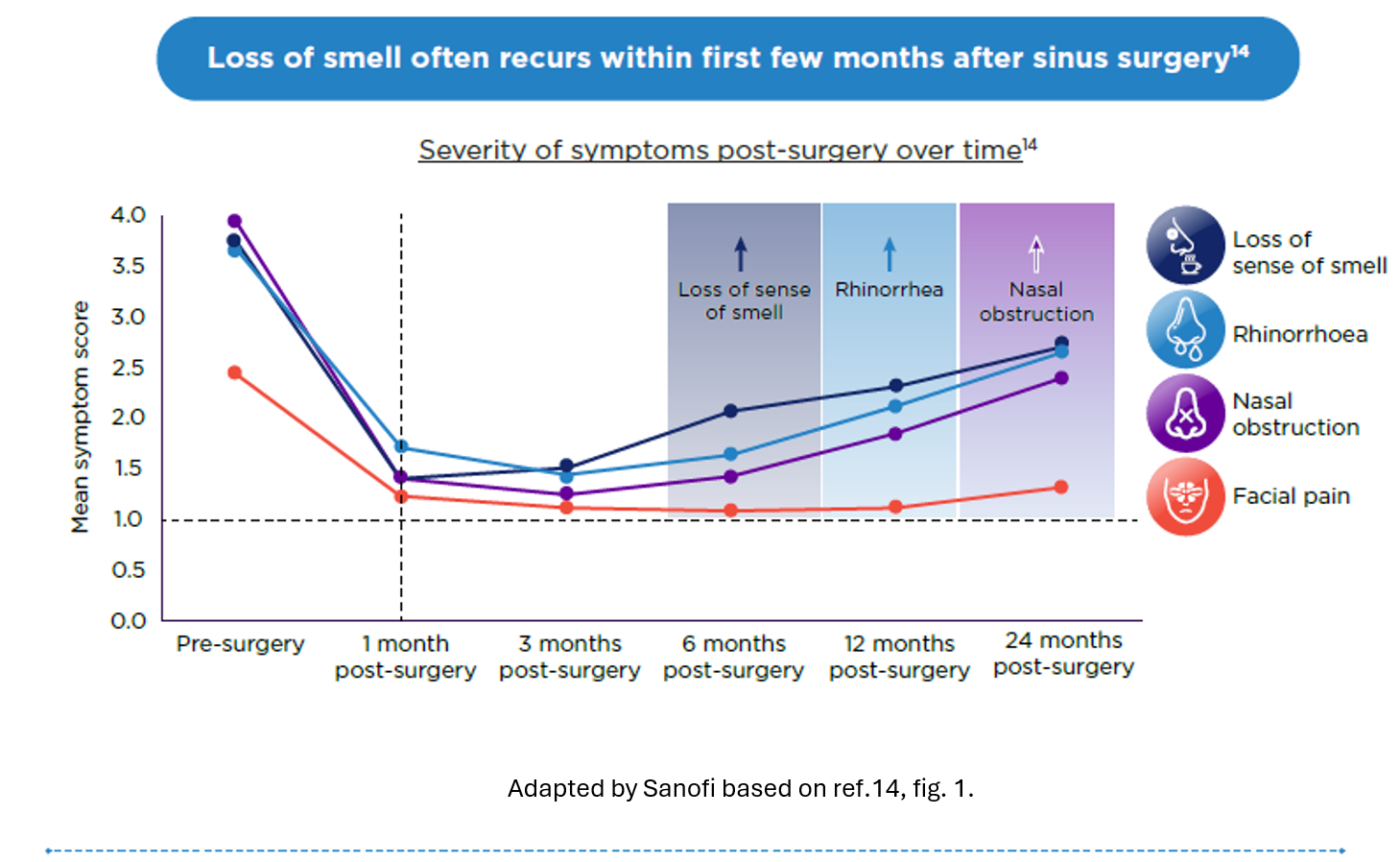
Recurrence of nasal polyps after surgical interventions remains a significant challenge in CRSwNP patients5 |
Recurrence of CRSwNP is defined as the persistence of postoperative endoscopic edema or polyps for more than one follow-up visit, lasting at least 3 months, requiring changes in treatment, and not attributable to concurrent upper respiratory infection.12 The presence of chronic type 2 inflammation may contribute to the recurrence of CRSwNP.2
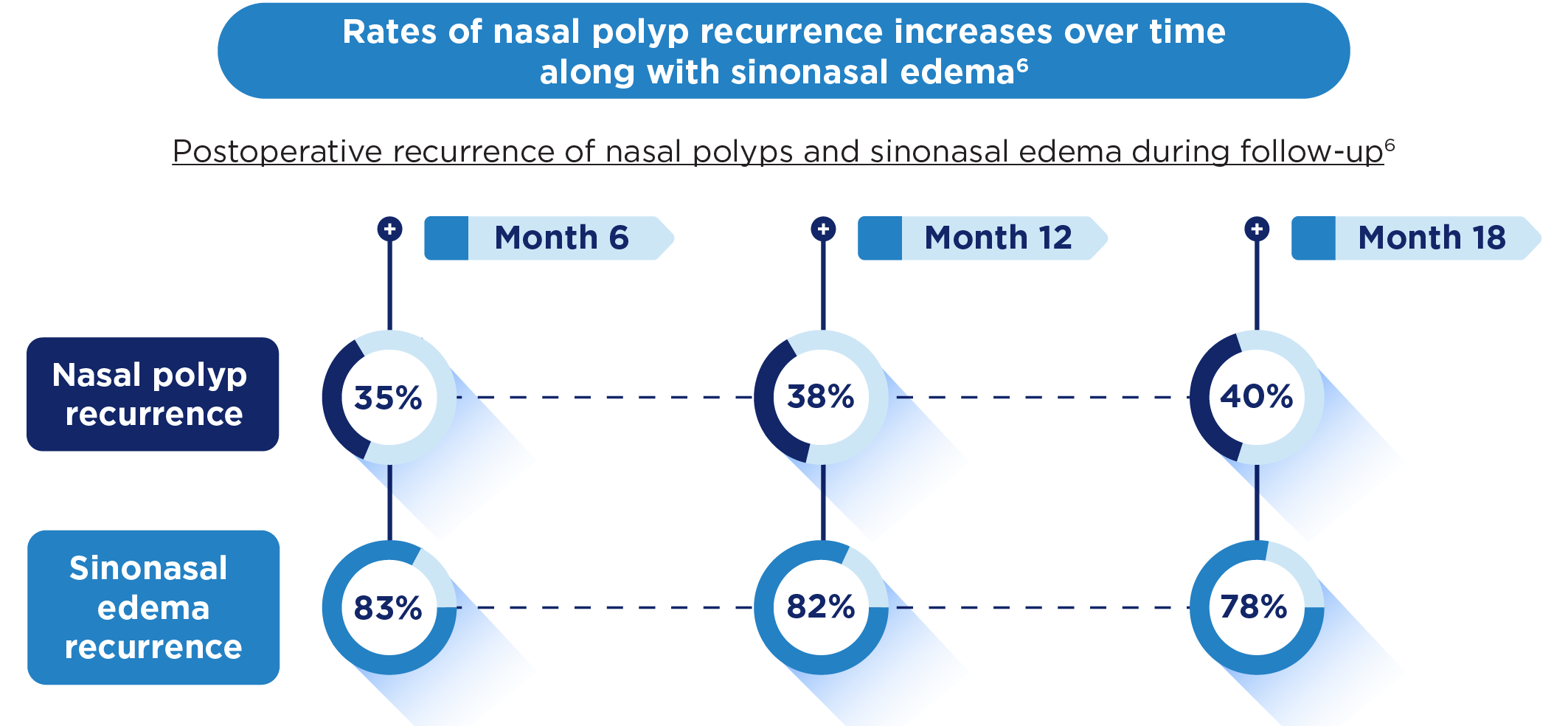
Recurrence of nasal polyps could be a function of untreated chronic inflammation5 |
Multimodal treatment approach is recommended for managing CRSwNP4,15

1st Line: INCS3,8,15,16
Long-term use reduces nasal polyp size and lowers the risk of recurrence after ESS.
2nd Line: SCS3,8,15–17
- No more than 1–2 courses annually.
- Recommended for severe exacerbations and partial/ uncontrolled condition.

Nasal Surgery8,16,18
- Removes nasal polyp tissue and diseased mucosa, improving airflow and symptom burden.
- Considered when medical treatments fail.
These treatments offer temporary relief but do not fully address type 2 inflammation, potentially leading to nasal polyp recurrence2,5–8
Guideline recommendation3,9
The EPOS 2020 and ICAR 2021 guidelines recommend biologics for those who do not respond to conventional therapies.

Biologic Therapy1,8,13,15,18
Targets type 2 inflammation, particularly those with severe or refractory disease.

Response to biologics is assessed by3
- Reduced nasal polyp.
- Decreased corticosteroid use.
- Improved smell and QoL.
CRSwNP, chronic rhinosinusitis with nasal polyps; EPOS, European Position Paper on Rhinosinusitis and Nasal Polyps; ESS, endoscopic sinus surgery; ICAR, International consensus statement on allergy and rhinology; IL, interleukin; INCS, intranasal corticosteroids; QoL, quality of life; SCS, systemic corticosteroids; SoC, standard of care.
-
Bachert C, et al. Front Immunol. 2024;15:1356298;
-
Maspero J, et al. ERJ Open Res. 2022;8(3):00576–2021;
-
Fokkens WJ, et al. Rhinology. 2020;58(Suppl 29):1–464;
-
De Corso E, et al. Acta Otorhinolaryngol Ital. 2023;43(Suppl. 1):S3-S13;
-
Bachert C, et al. J Asthma Allergy. 2021;14:127–134;
-
DeConde AS, et al. Laryngoscope. 2017;127(3):550–555;
-
Levi L, et al. Eur Arch Otorhinolaryngol. 2024;281(11):5847–5856;
-
Desrosiers M, et al. Rhinology. 2021;59(3):301–311;
-
Orlandi RR, et al. Int Forum Allergy Rhinol. 2021; 11(3):213–739;
-
Stevens WW, et al. J Allergy Clin Immunol Pract. 2019;7(8):2812–2820.e3;
-
Merrill T, et al. Clin Interv Aging. 2022; 17:685–698;
-
Cavaliere C, et al. J Pers Med. 2024;14(3):297;
-
Soler ZM, et al. Adv Ther. 2024;41(12): 4384–4395;
-
Bakhshaee M, et al. Iran J Otorhinolaryngol. 2016;28(85):125–134;
-
Han JK, et al. Int Forum Allergy Rhinol. 2021;11(10):1407–1416;
-
Gevaert P, et al. Int Forum Allergy Rhinol. 2022;12(11):1413–1423;
-
Rank MA, et al. Pol Arch Intern Med. 2023;133(11):16611;
-
Norelli F, et al. J Clin Med. 2024;13(4):1066.
Dette kan også være av interesse

Chronic Rhinosinusitis with Nasal Polyps: The Interplay of Type 2 Inflammation and Smell Loss


Loss of Smell in CRSwNP
Loss of sense of smell is a common symptom of chronic rhinosinusitis with nasal polyps (CRSwNP), but its impact is often underestimated. Learn how olfactory dysfunction affects patient’s quality of life and explore the underlying mechanisms driving smell loss in CRSwNP.