- Article
- Source: Campus Sanofi
Inflamación Tipo 2

.2024-03-05-11-25-14.svg)
¿Por Qué Es Importante Identificar La Inflamación De Tipo 2?
Prevalencia
~50%a a 70%b de los pacientes con asma tienen inflamación de tipo 2, afectando a un amplio espectro de pacientes1,2
aN=205 | bN=37
Heterogeneidad
1. Alérgico: IgE elevada y/o FeNO elevado.
2. Eosinofílico y Alérgico: IgE elevada y EOS elevados y/o FeNO elevado
3. Eosinofílico: EOS elevados y/o FeNO elevado
Clasificación
Criterios GINA para identificar la presencia de infla- mación de tipo 2 en las vías respiratorias4
EOS en sanáre ≥150 Células/uL y/o FeNO ≥20 ppb y/o Esputo EOS ≥2% y/o Asma provocada clínicamente por aleráenos
La Inflamación De Tipo 2 Es Un Factor De Riesgo Para Futuras Exacerbaciones5
Impacto en el paciente:
La inflamación de tipo 2 en asma está asociada a una carga elevada de la enfermedad4 6. Los pacientes con comorbilidades de tipo 2, incluida la RSC-PN, presentan una mayor caráa de la enfermedad7,8
- Asma mal controlada y exacerbaciones más frecuentes
- Mayor deterioro de la función pulmonar y aumento de la hiperreactividad bronquial
- Mayor exposición a OCS (> riesgo de efectos secundarios)
- Deterioro en la calidad de vida
RSC NP: rinosinusitis crónica con poliposis nasal | EOS:eosinófilos | FeNO:fracción de óxido nítrico exhalado | GINA:Iniciativa Global para el Asma | OCS:corticosteroides orales.
La inflamación de tipo 2 no abordada conduce a un inadecuado control de los síntomas y presenta un mayor riesgo de malos resultados terapéuticos4,5

Abordar Las Causas Clave De La Inflamación De Tipo 28
Ciencia e impacto
IL 4, IL-13, e IL-5 son responsables de la compleja fisiopatología del asma8-10
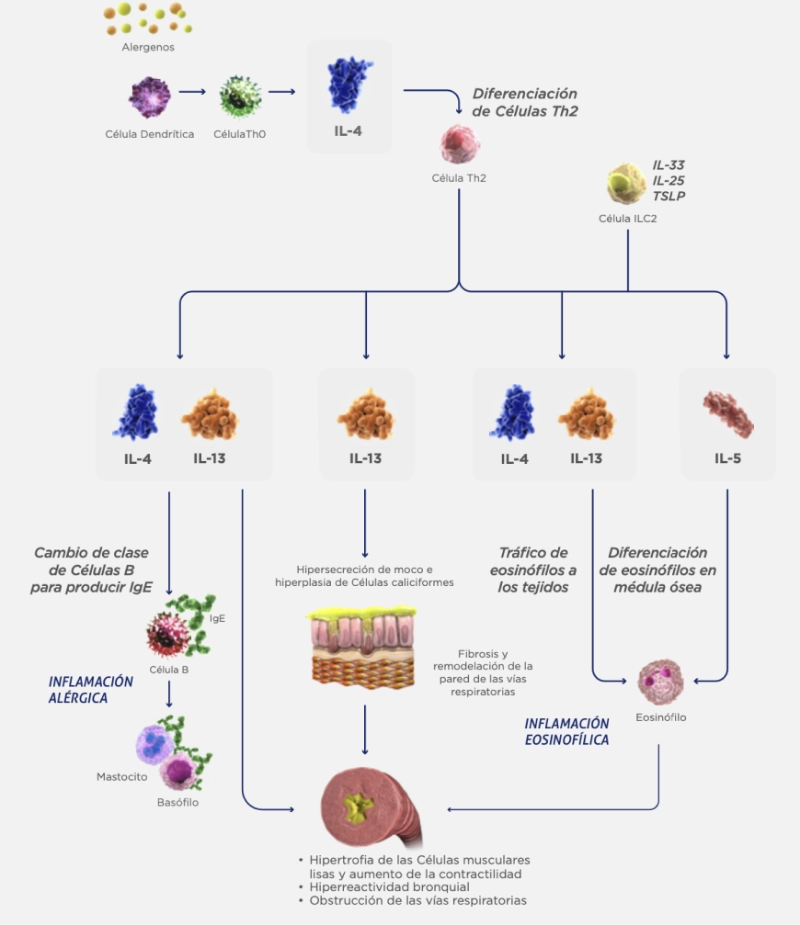
ILC2: Células linfoides innatas tipo 2 | TSLP: linfopoyetina estromal tímica.
IL-4 e IL-13 tienen roles clave con un amplio impacto sobre los síntomas del asma

IL-4 e IL-13 tienen un amplio impacto en la inflamación de tipo 28

Considerar El Amplio Impacto De La Inflamación De Tipo 2 Sobre Los Objetivos De Tratamiento4,5
El Desafío
La inflamación de tipo 2 es una entidad altamente hete rogénea con una fisiopatología compleja3,8

Múltiples fenotipos y biomarcadores

Múltiples Células inflamatorias
Los Objetivos
La inflamación tipo 2 obstaculiza los 4 objetivos clave de los tratamientos4,5
- Reducción de las exacerbaciones
- Mejoría y preservación de la función pulmonar
- Reducción del uso de OCS
- Mejoría de la calidad de vida de los pacientes
Se debe abordar y tratar la inflamación de tipo 2 en forma global para lograr un control óptimo del asma4,5
- Fahy JV. Type 2 inflammation in asthma — present in most, absent in many. Nat Rev lmmunol. 2015;15(1):57-65.
- Peters MC, Mekonnen ZK, Yuan S, Bhakta NR, Woodruff PG, Fahy JV. Measures of gene expression in sputum cells can iíentify TH2-high and TH2 low subtypes of asthma. J Allergy Clin Immunol. 2014;133(2):388-394.
- Rogliani P, Calzetta L, Matera MG, et al. Severe asthma and biological therapy: when, which, and for whom. Pulm Ther. 2019. doi:10.1007/s41030-019-00109-1
- Global Initiative for Asthma. Difficult to treat & severe asthma in adolescent and adult patients, 2020. https://ginasthma.org/wp content/uploaís/2020/04/ GINA-2020-full report_-final _wms.píf. Accessed April 13, 2020.
- Dunican EM, Fahy JV. The role of type 2 inflammation in the pathogenesis of asthma exacerbations. Ann Am Thorac Soc. 2015;12(suppl 2): S144 S149.
- Bai TR, Vonk JM, Postma DS, Boezen HM. Severe exacerbations predict excess lung function decline in asthma. Eur Resp J. 2007;30(3):452 456.
- Ceylan E, Gencer M, San I. Nasal polyps and the severity of asthma. Respirology. 2007;12(2):272 276.
- Gandhi NA, Bennett BL, Graham NM, Pirozzi G, Stahl N, Yancopoulos GD. Targeting key proximal drivers of type 2 inflammation in disease. Nat Rev Drug Discov. 2016;15(1):35-50.
- Robinson D, Humbert M, Buhl R, et al. Revisitng type 2-high and type 2 low airway inflammation in asthma: current knowleíge aní therapeutic implications. Clin Exp Allergy. 2017;47(2):161-175.
- Hammaí H, Lambrecht BN. Dendritic cells and epithelial cells: linking innate and adaptive immunity in asthma. Nat Rev lmmunol. 2008;8(3):193-204.
-(2).png/jcr:content/MAIN-TEXT%20(9)%20(2).png)
Mecanismos inflamatorios del asma: fisiopatología y relevancia clínica
Revisión de los principales mecanismos inflamatorios implicados en el asma, con foco en la activación del eje Th2/ILC2, las citocinas clave (IL-4, IL-5, IL-13), el reclutamiento eosinofílico, el remodelado de la vía aérea y los biomarcadores de inflamación tipo 2 aplicables a la práctica clínica para la fenotipificación y selección terapéutica.
-2.png/jcr:content/THUMBNAIL%206%20ASMA%20(2)-2.png)
Primer estudio de RWE sobre la efectividad de Dupilumab: Seguridad y relevancia en la práctica clínica
LA EFECTIVIDAD DE DUPILUMAB: SEGURIDAD Y RELEVANCIA EN LA PRÁCTICA CLÍNICA
.png/jcr:content/ASMA%205%20APP%20(2).png)
La efectividad de Dupilumab
PRIMER ESTUDIO DE RWE SOBRE LA EFECTIVIDAD DE DUPILUMAB: EL EFECTO DE LOS BIOMARCADORES IT2 (FENO)
perfiles-de-pacientes-lucas
.2024-03-12-15-52-14.svg)
Perfil clínico
- 16 años, diagnosticado hace 8 año
- Sufre de signos y síntomas intensos.
- Sufre de signos y síntomas intensos.
- Tratamiento actual: CET de alta potencia. Sin respuesta a fototerapia.
Impacto
- Las lesiones altamente visibles en el rostro tienen un impacto en su vida social.
- El prurito lo distrae durante las clases y no lo deja dormir por las noches.
- Tuvo siete ausencias escolares este año debido a la enfermedad.
- La enfermedad tiene, además, un impacto negativo en sus padres, incluido el estrés.
Metas del tratamiento
- Reducir el prurito.
- Mejorar las lesiones cutáneas.
- Distraerse menos en la escuela a causa de sus síntomas.
perfiles-de-pacientes-sofia

Perfil clínico
- 26 años, diagnosticada en la primera infancia.
- Ha sufrido erupciones problemáticas y trastornos frecuentes del sueño.
- Mejora clínica inadecuada con el tratamiento actual.
- Tratamiento actual: CET. Debió suspender ciclosporina por efectos adversos.
Impacto
- Lesiones cutáneas en las áreas de flexión.
- El prurito persistente provoca trastornos del sueño.
- El prurito persistente provoca trastornos del sueño.
Metas del tratamiento
- Reducir el prurito.
- Mejorar las lesiones cutáneas.
- Encontrar un tratamiento que permita un control adecuado a largo plazo de su enfermedad sin toxicidad.
perfiles-de-pacientes-mateo

Perfil clínico
- 50 años, diagnosticado en la primera infancia.
- No logra sostener el control a largo plazo de la enfermedad con el tratamiento actual
- Tratamiento actual: CET y ciclosporina, con pobre respuesta.
Impacto
- Lesiones crónicas: liquenificación con sobre-infecciones frecuentes.
- Prurito severo persistente.
- La pérdida frecuente del sueño afecta el desempeño laboral.
Metas del tratamiento
- Lesiones crónicas: liquenificación con sobre-infecciones frecuentes.
- Prurito severo persistente.
- La pérdida frecuente del sueño afecta el desempeño laboral.