Beyfortus®▼(nirsevimab): effectiveness and public health impact in the real world

▼ This medicinal product is subject to additional monitoring.
Beyfortus® is indicated for the prevention of Respiratory Syncytial Virus (RSV) lower respiratory tract disease in:1
- Neonates and infants during their first RSV season;
- Children up to 24 months of age who remain vulnerable to severe RSV disease through their second RSV season.
Beyfortus® should be used in accordance with official recommendations.1
Beyfortus® has an unparalleled body of real-world evidence against RSV disease, including hospitalizations2–60
> 50 real-world studies in over 400,000 Beyfortus®-immunized infants across the Northern and Southern Hemispheres*,2-60 |

A meta-analysis of 27 studies assessed the effectiveness of Beyfortus® against RSV-related outcomes in the real world61
The 27 studies included after screening/eligibility, was conducted in Spain, France, US, Italy and Luxembourg. Beyfortus® was associated with high effectiveness against RSV-related outcomes61:
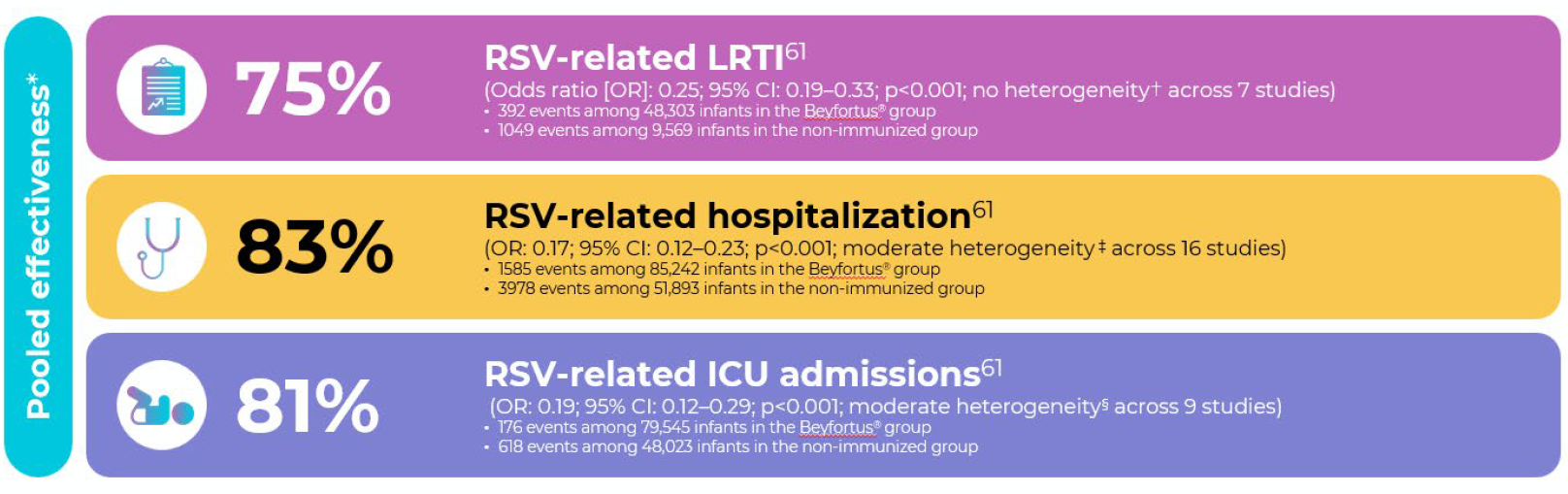
Length of hospital stay: No difference between Beyfortus®-immunized infants and non-immunized infants was observed (weighted mean difference [WMD]: 0.10; 95% CI: -0.63–0.65; p=0.97)
The NIRSE-GAL study: A real-world effectiveness and impact study from Galicia, Spain60
Galicia, a region in northwestern Spain, became one of the first places in the world to introduce nirsevimab as part of its regional immunization program for infants. The study was conducted between September 25, 2023, and ended March 31, 2024. It included over 13,300 infants.2,60
After Beyfortus® implementation, RSV LRTI hospitalization decreased substantially by 89,2%¶ vs. five previous seasons for infants in the overall cohort (infants born before and during RSV season).60 |
In this real-world study, high coverage was achieved in the seasonal and catch-up groups. High effectiveness and public health impact were seen with Beyfortus. The findings from this study support clinical trial efficacy and safety data.1,60,62,63
Watch the video below to learn more about the findings of the study:

The data in the video are expressed as relative risk reduction, while the corresponding absolute risk reduction is not reported in the manuscript.
▼Beyfortus had a favorable safety profile in clinical trials.1,62-65
Safety has been studied in a broad population, including healthy premature infants and children at higher risk of RSV infections of the lower respiratory tract. The type and frequency of adverse reactions with Beyfortus were comparable to placebo in the Phase 2b and Phase 3 studies.1,62-65

Rash
within 14 days of dosing

Pyrexia
within 7 days of dosing

Injection site reactions
within 7 days of dosing
Hypersensitivity reactions have been spontaneously reported after marketing authorisation; The frequency is unknown.1
In the study in infants at higher risk of severe RSV, the safety profile of Beyfortus was comparable to that of the comparator medicinal product palivizumab and consistent with the safety profile of nirsevimab in full-term and preterm infants at GA ≥ 29 weeks.1,62,65
* In Andorra, Australia, Chile, France, Italy, Luxembourg, Portugal, Spain, and the United States as of August 05, 2025.
** Results are reported as OR and WMD with 95% CIs. Statistical heterogeneity across studies was assessed using the I² and 𝜏𝜏² metrics; I2 values of 0–40% indicate low heterogeneity, 41–75% indicate moderate heterogeneity, and values greater than 75% indicate high heterogeneity.60 Tau2 (𝜏𝜏2 ) is the variance of the effect size parameters across the population of studies and reflects the variance of the true effect sizes.
† I2 = 0.0%; 𝜏𝜏2 = 0.000.
‡ I2 = 65.3%; 𝜏𝜏2 = 0.186.
§ I2 = 58.6%; 𝜏𝜏2 = 0.235. 60
¶ IQR: 89.1–91.4%.
▼This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions.
Beyfortus® (nirsevimab) – Compulsory Information
Presentation: Beyfortus 50 mg and 100 mg solution for injection in pre-filled syringe containing 50 mg of nirsevimab in 0.5 mL (100 mg/mL) and 100 mg of nirsevimab in 1 mL (100 mg/mL) respectively. Nirsevimab is a human immunoglobulin G1 kappa (IgG1K) monoclonal antibody produced in Chinese hamster ovary (CHO) cells by recombinant DNA technology. This medicine contains 0.1 mg of polysorbate 80 (E433) in each 50 mg (0.5 mL) dose and 0.2 mg in each 100 mg (1 mL) dose.
Indication: Prevention of Respiratory Syncytial Virus (RSV) lower respiratory tract disease in neonates and infants during their first RSV season, and children up to 24 months of age who remain vulnerable to severe RSV disease through their second RSV season. Beyfortus should be used in accordance with official recommendations. Dosage and administration: For infants during their first RSV season, the recommended dose is a single dose of 50 mg for infants with body weight <5 kg or 100 mg for infants ≥5 kg, administered intramuscularly. Beyfortus should be administered from birth for infants born during the RSV season. For others born outside the season Beyfortus should be administered ideally prior to the RSV season. Dosing in infants with a body weight from 1.0 kg to <1.6 kg is based on extrapolation, no clinical data are available. Exposure in infants <1 kg is anticipated to yield higher exposures than in those weighing more. The benefits and risks of nirsevimab use in infants <1 kg should be carefully considered. There are limited data available in extremely preterm infants (Gestational Age [GA] <29 weeks) less than 8 weeks of age. No clinical data available in infants with a postmenstrual age (gestational age at birth plus chronological age) of less than 32 weeks. For children who remain vulnerable to severe RSV disease through their second RSV season, the recommended dose is a single dose of 200 mg given as two intramuscular injections (2 x 100 mg).
Beyfortus should be administered ideally prior to the start of the second RSV season. For individuals undergoing cardiac surgery with cardiopulmonary bypass, an additional dose may be administered as soon as the individual is stable after surgery to ensure adequate nirsevimab serum levels. If within 90 days after receiving the first dose of Beyfortus, the additional dose during the first RSV season should be 50 mg or 100 mg according to body weight, or 200 mg during the second RSV season. If more than 90 days have elapsed since the first dose, the additional dose could be a single dose of 50 mg regardless of body weight during the first RSV season, or 100 mg during the second RSV season, to cover the remainder of the RSV season. Safety and efficacy in children 2-18 years not established.
Beyfortus is for intramuscular injection only, preferably in the anterolateral aspect of the thigh. Gluteal muscle should not be used routinely due to risk of sciatic nerve damage. If two injections are required, different injection sites should be used. Contraindication: Hypersensitivity to the active substance or to any of the excipients. Warnings and precautions: To improve traceability of biological medicinal products, record the name and batch number. Serious hypersensitivity reactions, have been reported following Beyfortus administration. Anaphylaxis has been observed with human immunoglobulin G1 (IgG1) monoclonal antibodies. If signs and symptoms of anaphylaxis or other clinically significant hypersensitivity reaction occur, immediately discontinue administration and initiate appropriate medicinal products and/or supportive therapy. As with any other intramuscular injections, nirsevimab should be given with caution to individuals with thrombocytopenia or any coagulation disorder. In some immune compromised children with protein-losing conditions, a high clearance of nirsevimab has been observed in clinical trials, and nirsevimab may not provide the same level of protection in those individuals. This medicine contains 0.1 mg of polysorbate 80 in each 50 mg (0.5 mL) dose and 0.2 mg in each 100 mg (1 mL) dose. Polysorbates may cause allergic reactions. Interactions: Nirsevimab can be given concomitantly with childhood vaccines. Nirsevimab should not be mixed with any vaccine in the same syringe or vial. When administered concomitantly with injectable vaccines, they should be given with separate syringes and at different injection sites. Fertility, Pregnancy and Lactation: Not applicable. Undesirable effects: Adverse reactions reported in clinical trials are uncommon: rash, injection site reaction, and pyrexia. For a complete list of undesirable effects please refer to the Summary of Product Characteristics. Health care professionals are asked to report any suspected adverse reactions via their national reporting system. Marketing Authorisation Holder: Sanofi Winthrop Industrie, 82 avenue Raspail, 94250 Gentilly, France. Legal Classification of the medicinal product regarding medical prescription: Prescription Only Medicine. Date of last review: 25.04.2025.
Abbreviated Prescribing Information based on the EU SmPC as of April 2025.
Before prescribing the product always refer to your full local prescribing information as this information may vary from country to country.
SWEDEN: Beyfortus (nirsevimab). Rx, EF, J06BD
For complete prescriber information, see www.fass.se. Contact details: Beyfortus is provided by Sanofi AB. Box 300 52, 10425 Stockholm, tel +46 8 634 50 00. For questions about our medicines, contact: infoavd@sanofi.com. Date of revision of the summary of product characteristics: 04/2025
-
Beyfortus®. EU Summary of Product Characteristics (SmPC) April 2025.
-
Ares-Gómez S et al. Lancet Infect Dis 2024; 24(8): 817–828.
-
Ernst C et al. Euro Surveill 2024; 29(4): 2400033.
-
Ezpeleta G et al. Vaccines 2024; 12(4): 383.
-
López-Lacort M et al. Euro Surveill2024; 29(6): 2400046.
-
PaireauJ et al. Influenza OtherRespirViruses2024; 18(6): e13311.
-
MazagatosC et al. Influenza OtherRespViruses2024; 18(5): e13294.
-
ConsolatiA et al. Vaccines 2024; 12(5): 549.
-
Estrella-Porter P et al. Vaccines 2024; 42(22): 126030.
-
Levy C et al. J PediatrInfect Dis Soc 2024; 13(7): 371–373.
-
Coma E et al. Arch Dis Child 2024; 109(9): 736–741.
-
AgüeraM et al. Pediatr Allergy Immunol 2024; 35(6): e14175.
-
Assad Z et al. N Engl J Med 2024; 391(2): 144–154.
-
Molina Gutierrez MA et al. EnfermInfeccMicrobiolClin (EnglEd) 2024; 42(7): 367–372.
-
Lassoued Y et al. Lancet Reg Health Eur 2024; 44: 101007.
-
Barbas Del Buey JF et al. Front Public Health 2024; 12: 1441786.
-
Pérez Martín JJ and Moreno MZ. Human Vaccines Immunother 2024; 20(1): 2365804.
-
García-García ML et al Authorea 2024. https://doi.org/10.22541/au.172464773.33348406/v1. [Epub ahead of print].
-
Carbajal R et al. Lancet Child Adolesc Health 2024; 8: 730–739.
-
Martinez DA et al. Pediatrics 2024; 154(4): e2024066584.
-
Xu H et al. JAMA Netw Open 2025; 8(3): e250380.
-
Jimeno Ruiz S et al. Vaccines 2024; 12: 1160.
-
López-Lacort M et al. Pediatrics2025; 155(1): e2024066393.
-
Perramon-MalavezA et al. Euro J Pediatr2024; 183: 5181–5189.
-
Reina J. EnfermInfeccMicrobiolClin 2023; 41: 301–304.
-
RazzaghiH et al. MMWR MorbMortal WklyRep. 2024; 73(38): 837–843.
-
HsiaoA et al. Annals Allergy Asthma Immunol 2024; 133(6;Supple2): S3–S4.
-
Lefferts B et al. Morbidity and Mortality Weekly Report 2024; 73(45): 1015–1021.
-
JeziorskiE et al. PediatrInfect Dis J 2024; 44(4): e124–e126.
-
Askari MS et al. Morbidity and Mortality Weekly Report 2024; 73(48): 1107–1109.
-
De Sentuary CO et al. EClinicalMedicine2024; 79: 102986.
-
Moline HL et al. JAMA Pediatr 2025; 179-187.
-
Chauvel C et al. Influenza Other Respi Viruses 2024; 18: e70054.
-
Ma KSK et al. Pediatr Res 2025. doi: 10.1038/s41390-024-03782-4. [Epub ahead of print].
-
CarcioneD et al. PediatrInfect Dis J 2025. doi: 10.1097/INF.0000000000004715. [Epub ahead of print].
-
Perramon-Malavez A et al. Pediatr Infect Dis J 2025. doi: 10.1097/INF.0000000000004672. [Epub ahead of print].
-
Cavaco Afonso AF et al. Authorea 2025. doi: 10.22541/au.173780129.99727424/v1. [Epub ahead of print].
-
LenglartL et al. EurJ Pediatr2025; 184(2):171.
-
NúñezO et al. Euro Surveill2025; 30(5): 2400596.
-
LitmanA et al. JAMA NetwOpen 2025; 8(2): e2460729.
-
JabagiMJ et al. NEJM Evid2025; 4(3): doi: 10.1056/EVIDoa2400275.
-
Moreno-Pérez D et al. Vaccines 2025; 13(2): 175.
-
Pastor-Barriuso R et al. Euro Surveill 2025; 30(6): 2500040.
-
Blauvelt CA et al. JAMA Net Op 2025; 8(2): e2460735.
-
Marouk A et al. Eur J Pediatr 2025; 184(3): 229.
-
Wadia U et al. J Infect 2025; 90(4): 106466.
-
Rius-Peris JM et al. Acta Paediatr 2025; 114(8): 1963–1976.
-
Touati S et al. Ann Intensive Care 2025; 15(1): 56.
-
Irving SA et al. Pediatrics2025; 155(6): e2024070240.
-
Silva-Afonso RF et al. EnfermInfeccMicrobiolClin (EnglEd) 2025; 43(7): 435–443.
-
Coma E et al. Arch Dis Child Published online June 10, 2025. doi:10.1136/archdischild-2025-329005
-
Alejandre C et al. Eur J Pediatr2024: 183(9): 3897–3904.
-
Cantais A et al. J Med Virol 2024; 96(2): e29483.
-
Espeleta-Fox A et al. Pediatr Pulmonol 2024; 59(12): 3783-3786.
-
Homo RL et al. J Pediatr 2024; 273: 114144.
-
Kemp M et al. Vaccine 2025; 47: 126674.
-
Puckett L et al. Hosp Pediatr 2025; 15(2): 99–107.
-
Bermúdez-Barrezueta L et al. Eur J Pediatr 2025; 184(6): 345.
-
Torres JP et al. Lancet Infect Dis Published online June 10, 2025. doi:10.1016/S1473–3099(25)00233-6.
-
Mallah N et al. Lancet Infect Dis 2024:S1473-3099(24)00811-9 & Supplementary Appendix.
-
Sumsuzzman D et al. Real-world effectiveness of nirsevimab against respiratory syncytial virus disease in infants: a systematic review and meta-analysis. The Lancet Child Adolesc Health, 9 (2025), pp. 393-403.
-
Griffin MP et al. N Eng J Med 2020; 383(5): 415–425.
-
Hammitt LL et al. N Engl J Med 2022; 386(9): 837–846.
-
Drysdale SB et al. N Engl J Med 2023; 389(26): 2425–2435.
-
Domachowske J et al. N Engl J Med 2022; 386(9): 892-894
Relaterade Artiklar

RSV-prevention med Beyfortus (nirsevimab) – tillgänglig för nyfödda från 10 september
Beyfortus® är en RSV-immunisering designad för alla spädbarn, för skydd mot RSV-sjukdom i de nedre luftvägarna (LRTD).1
SE-FILMEN-HÄR
