
Why Dupixent
Conventional therapies may not be enough
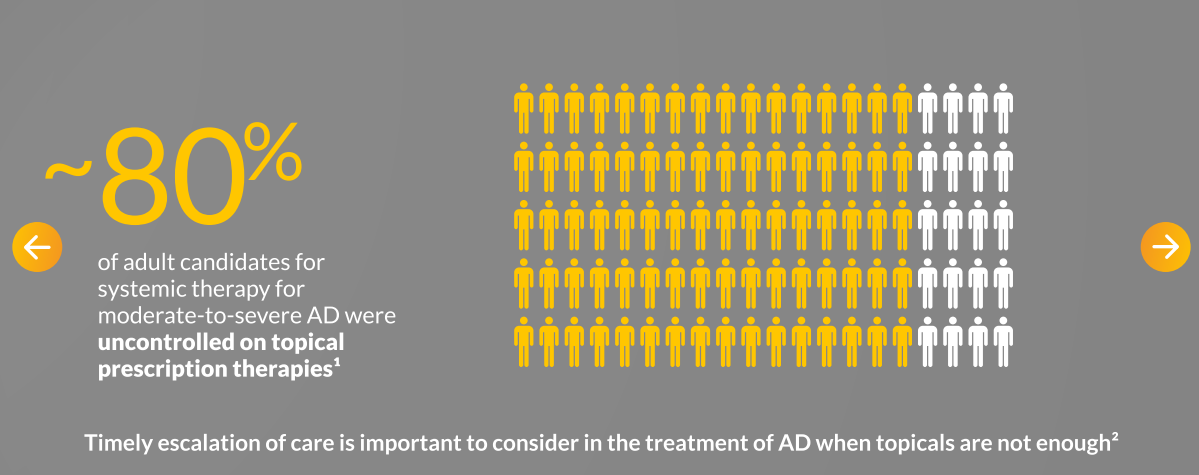
TOO MANY PATIENTS ARE LIVING with UNCONTROLLED SKIN CONDITIONS DRIVEN BY TYPE 2 INFLAMMATION3,4…
With long-term consequences beyond what they feel and see on their skin5-8
Precisely Targeted, Continuously Controlled |

DUPIXENT is the first and only dual inhibitor of IL-4 and IL-13 signaling, targeting an important mechanism of inflammation common across a range of skin diseases1

DUPIXENT reduces itch from the first dose, clears skin, and improves quality of life, achieving long-term control beyond itch and skin1,9,10

DUPIXENT has a consistent safety profile across a range of patients, from infants to the elderly, in AD1
Improve life quality beyond itch with DUPIXENT: Target type 2 inflammation in AD early for rapid and sustained relief in itch, skin, and long-term quality of life1,9,10 |
More than 1 MILLION PATIENTS ON THERAPY WORLDWIDE across all indications1,2

ATOPIC DERMATITIS1
moderate-to-severe in 12+ years; severe in 6 months to 11 years who are candidate for systemic therapy
PRURIGO NODULARIS1
moderate-to-severe who are candidates for systemic therapy
CSU1
moderate-to-severe with inadequate response to H1 antihistamines and naive to anti-IgE therapy

ASTHMA1
add-on maintenance treatment for severe asthma with type 2 inflammation characterised by raised blood eosinophils and/or raised fraction of exhaled nitric oxide (FeNO), who are inadequately controlled with high dose inhaled corticosteroids (ICS) plus another medicinal product for maintenance treatment

CRSwNP1
add-on therapy with intranasal corticosteroids for the treatment of adults with severe CRSwNP for whom therapy with systemic corticosteroids and/or surgery do not provide adequate disease control

EoE1
in patients aged 1 year and older, weighing at least 15 kg, who are inadequately controlled by, are intolerant to, or who are not candidates for conventional medicinal therapy

COPD1
add-on maintenance treatment for uncontrolled chronic obstructive pulmonary disease (COPD) characterised by raised blood eosinophils on a combination of an inhaled corticosteroid (ICS), a long-acting beta2-agonist (LABA), and a long-acting muscarinic antagonist (LAMA), or on a combination of a LABA and a LAMA if ICS is not appropriate
Footnotes
a > 1,000,000 patients on therapy worldwide across all approved indications: AD, asthma, CRSwNP, PN, EoE, CSU, and COPD.2
Abbreviations
AD, atopic dermatitis; COPD, chronic obstructive pulmonary disease; CRSwNP, chronic rhinosinusitis with nasal polyposis; CSU, chronic spontaneous urticaria; EoE, eosinophilic esophagitis; IL, interleukin; OCS, oral corticosteroid; PN, prurigo nodularis.
References
-
DUPIXENT Summary of Product Characteristics, 11/2025.
-
IQVIA/Sanofi Integrated DUPIXENT platform, data through April 2025.
-
Staumont-Sallé D et al. Acta Derm Venereol. 2021;101(12):adv00618.
-
Todberg T et al. Acta Derm Venereol. 2020;100(8):adv00119.
-
von Stülpnagel CC et al. J Eur Acad Dermatol Venereol. 2021;35(11):2166-2184.
-
Pereira MP et al. Acta Derm Venereol. 2021;101(2):adv00403.
-
Aggarwal PV et al. Clin Exp Dermatol. 2021;46(7):1277-1284.
-
Rodriguez D et al. JAMA Dermatol. 2023;159(11):1205-1212.
-
Blauvelt A et al. Lancet. 2017;389(10086):2287-2303.
-
Silverberg JI et al. Acta Derm Venereol. 2021;101(11):adv00585.
-
Davis DMR et al. J Am Acad Dermatol. 2024;90(2):e43-e56.
-
Chu DK et al. Ann Allergy Asthma Immunol. 2024;132(3):274-312.
-
Werfel T et al. J Dtsch Dermatol Ges. 2024;22(2):307-320.
-
Wollenberg A et al. European Dermatology Forum. Living EuroGuiDerm Guideline for the Systemic Treatment of Atopic Eczema. Accessed June 13, 2025. https://www.guidelines.edf.one/guidelines/atopic-ezcema
Disease burden
Unmet needs
ARE YOUR PATIENTS WITH UNCONTROLLED AD SHARING THE FULL IMPACT OF THEIR DISEASE?
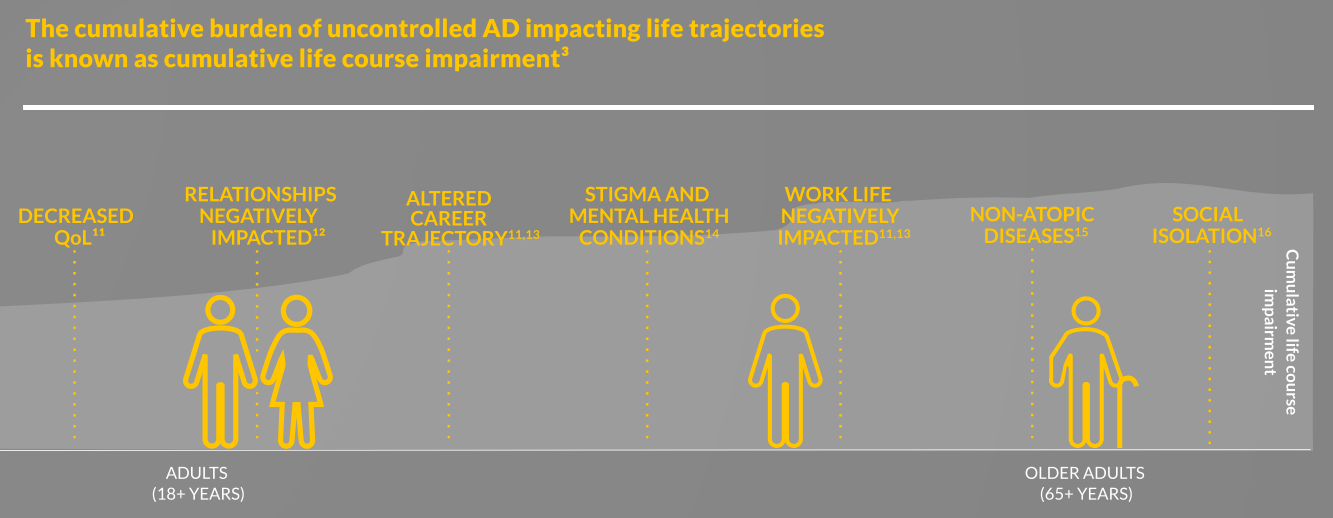
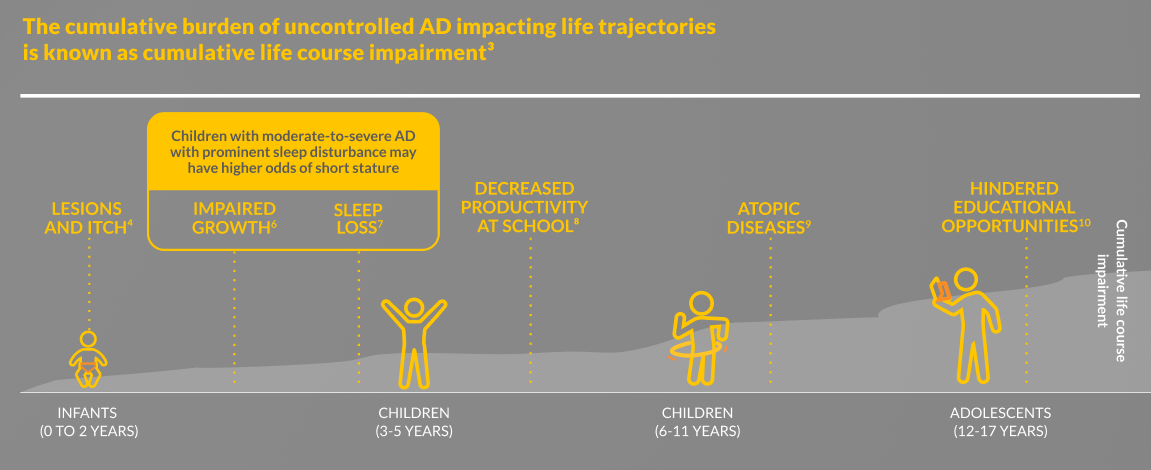
THE CONTINUOUS BURDEN OF UNCONTROLLED AD CAN ACCUMULATE OVER TIME3
THE CONTINUOUS BURDEN OF UNCONTROLLED AD CAN ACCUMULATE OVER TIME3
THE CONTINUOUS BURDEN OF UNCONTROLLED AD CAN ACCUMULATE OVER TIME3
THE CONTINUOUS BURDEN OF UNCONTROLLED AD CAN ACCUMULATE OVER TIME3
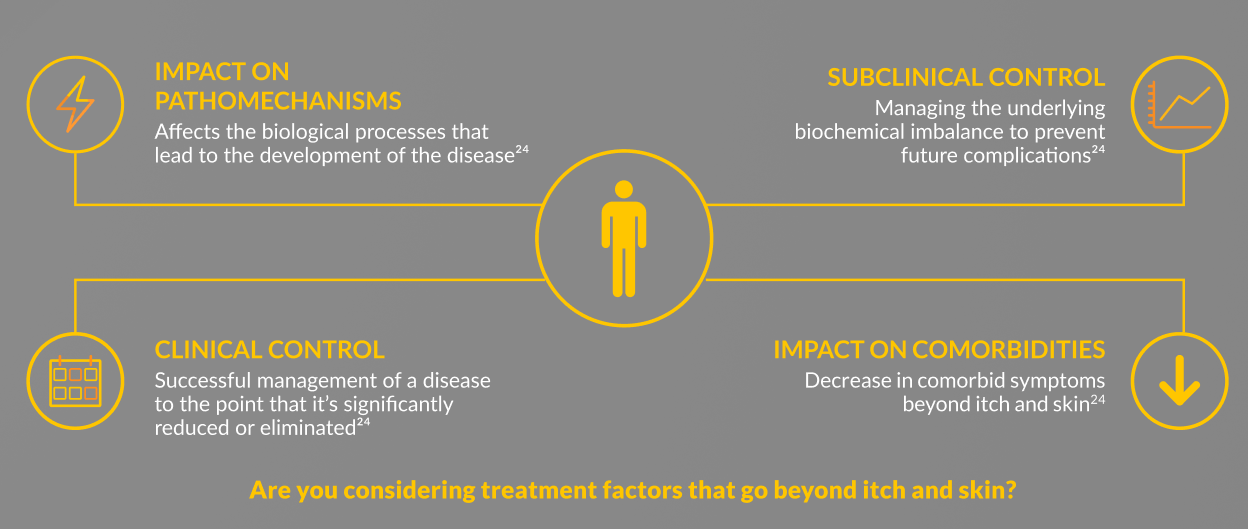
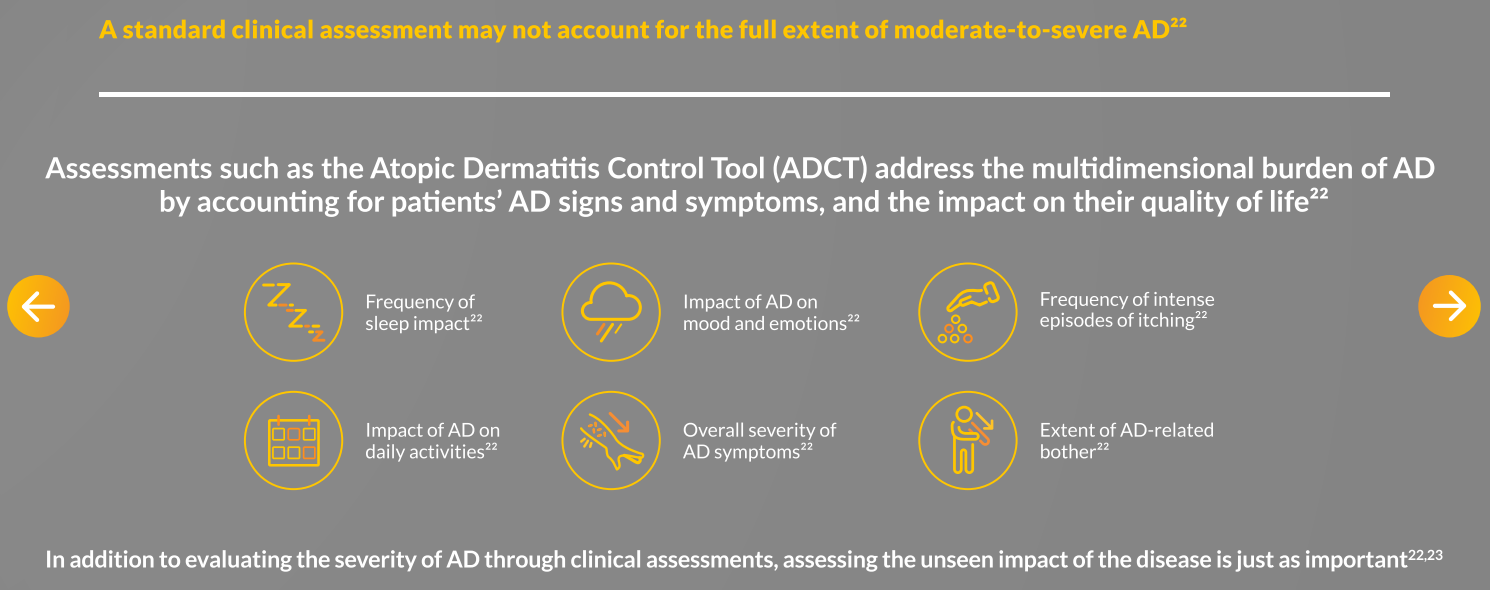
THE UNDERSTANDING OF AD BURDEN HAS EVOLVED BEYOND JUST THE CLINICALLY MEASURABLE IMPACT ON ITCH, SKIN, AND QoL24
WHICH UNCONTROLLED PATIENTS HAVE YOU SEEN IN YOUR PRACTICE?

Child
“It’s hard to watch him suffer every day. We’re concerned about the constant itch affecting his sleep.”

Adolescent
“I’m concerned that if I stay on topical steroids, I’ll start to see stretch marks on my skin.”

Adult
“I’m ready to try anything to get the flares under control and start getting better sleep.”

Adult
“I’m willing to consider any options that can help improve my overall skin health and my feelings of anxiety.”
Hypothetical atopic dermatitis cases. Not real patients.

AD impact could include:5,6
- Severe itch and lesions are affecting his sleep
- His parents feel overwhelmed, and are anxious that uncontrolled AD could affect his sleep and possibly even his rate of growth
Typical disease history could include:
- Progressively worsening itch and lesions from 6 months old
- Severe AD remains uncontrolled despite many cycles of topical treatments
Treatment Goals
“As his parents, we want to get this condition under control as soon as possible so he can play and live a normal life.” |

AD impact could include:5
- Persistent itching is making her lose sleep and fall behind in class
- Embarrassed that classmates and coworkers will notice only her moderate lesions
Typical disease history could include:
- Uncontrolled moderate AD despite multiple TCS cycles, including high-potency steroids, of three- to four-week periods
- Topical treatments not providing consistent relief from her underlying condition, and anxious about their possible long-term side effects
Treatment Goals
“I want a future free from flares, but I also want to avoid stretch marks and withdrawal signs and symptoms that can come from topical steroid use.” |

AD impact could include:5
- AD flares limit her social life, and poor sleep is causing problems at work
- She feels overwhelmed by the unpredictability of the flares, and the cascading consequences of poor sleep feel out of her control
Typical disease history could include:
- Has suffered from AD since childhood, and her relationships have long been affected by the embarrassment of flares
- Initial treatment with topical steroids stabilized her condition, but it has worsened over time with more frequent breakthrough flares
Treatment Goals
“I want to live my life worrying less about flares and how much they are affecting my sleep.” |

AD impact could include:5
- Visible lesions and lack of sleep are negatively impacting his mood and his relationships with work clients
- Has been frustrated with infections due to his AD
Typical disease history could include:
- Has suffered from moderate AD since early adulthood, has dealt with AD-related anxiety and depression, and is worried about infection risks
- Currently uncontrolled on optimized topical steroids; concerned about taking a systemic treatment long term
Treatment Goals
“I have a lot of AD-related anxiety and skin infections, and I’m looking for a treatment that can improve my overall skin health.” |
Abbreviations
AD, atopic dermatitis; EASI, Eczema Area and Severity Index; QoL, quality of life; RWE, real-world evidence; TARC, thymus and activation-regulated chemokine; TCI, topical calcineurin inhibitors; TCS, topical corticosteroids.
References
-
Eyerich K et al. J Eur Acad Dermatol Venereol. 2024;38(2):340-353.
-
Chovatiya R, Silverberg JI. Am J Clin Dermatol. 2022;23(4):459-468.
-
von Stülpnagel CC et al. J Eur Acad Dermatol Venereol. 2021;35(11):2166-2184.
-
Weidinger S et al. Nat Rev Dis Primers. 2018;4(1):1.
-
Augustin M et al. J Eur Acad Dermatol Venereol (JEADV). 2022;36(7):3-16.
-
Silverberg JI, Paller AS. JAMA Dermatol. 2015;151(4):401-409.
-
Paller AS et al. Lancet. 2022;400(10356):908-919.
-
Weidinger S et al. Br J Dermatol. 2024;190(6):846-857.
-
Irvine AD, Mina-Osorio P. Br J Dermatol. 2019;181(5):895-906.
-
Fasseeh AN et al. Dermatol Ther (Heidelb). 2022;12(12):2653-2668.
-
Bashyam AM et al. Dermatol Ther (Heidelb). 2021;11(3):1065-1070.
-
Silverberg JI et al. Ann Allergy Asthma Immunol. 2018;121(3):340-347.
-
Thaçi D et al. Dermatol Ther (Heidelb). 2022;12(9):2145-2160.
-
Long Q et al. PLoS One. 2022;17(2):e0263334.
-
von Kobyletzki L et al. J Eur Acad Dermatol Venereol. 2024;38(2):354-364.
-
Tanei R, Hasegawa Y. Geriatr Gerontol Int. 2016;16 Suppl 1:75-86.
-
Lugović-Mihić L et al. Pharmaceuticals (Basel). 2024;17(11):1455.
-
Merola JF et al. J Am Acad Dermatol. 2021;84(2):495-497.
-
Abuabara K et al. Dermatol Clin. 2017;35(3):291-297.
-
Bieber T. Nat Rev Drug Discov. 2022;21(1):21-40.
-
Haddad E-B et al. Dermatol Ther (Heidelb). 2022;12(7):1501-1533.
-
Pariser DM et al. Curr Med Res Opin. 2020;36(3):367-376.
-
Fishbein AB et al. J Allergy Clin Immunol Pract. 2020;8(1):91-101.
-
Bieber T. Ann Allergy Asthma Immunol. 2025;134(2):144-150.
MOD/MOA
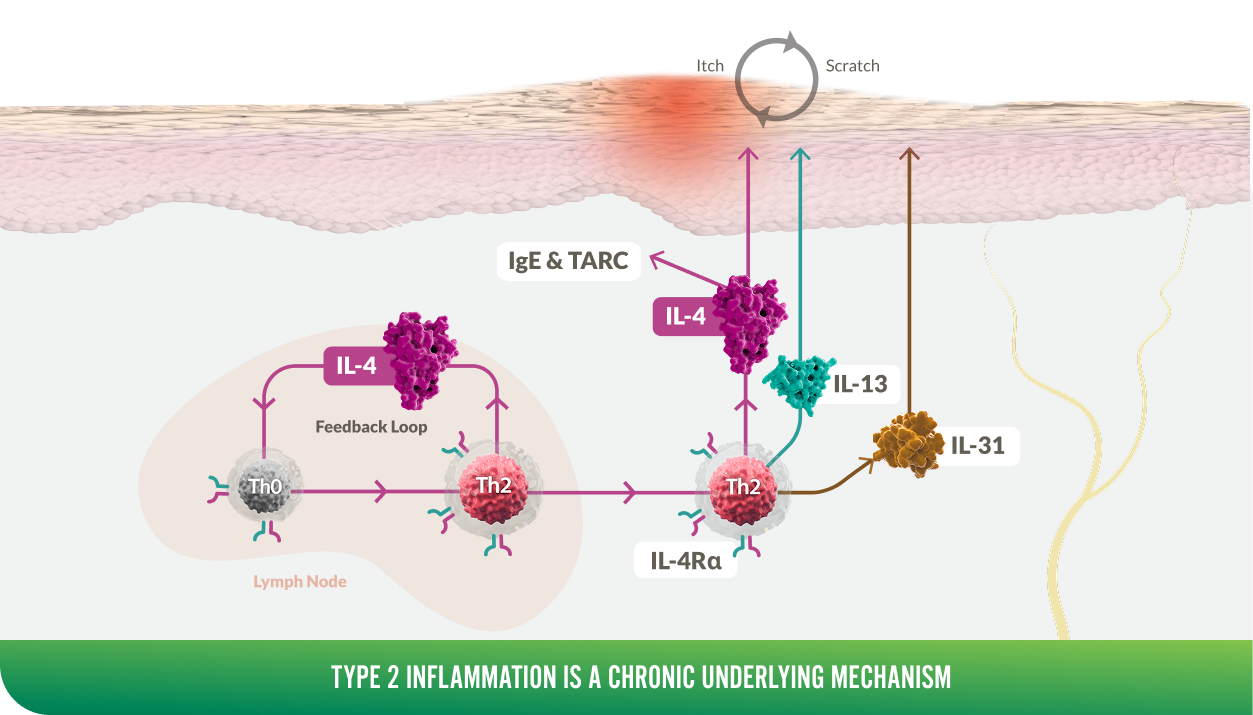
TWO KEY DRIVERS OF TYPE 2 INFLAMMATION, IL-4 AND IL-13, SIGNAL THROUGH IL-4Rα |
IL-4 is a key upstream modulator of Th2 response, promoting a positive feedback loop that contributes to increased secretion of IL-4, IL-13, and IL-311-7,a
IL-4 and IL-13 play overlapping yet distinct roles in type 2 inflammation8
Dysregulation of IL-4 and IL-13 signaling in the immune system of patients with AD leads to:
SKIN |
SENSORY NEURONS |
FLARES |
|
|
|
|
||
|
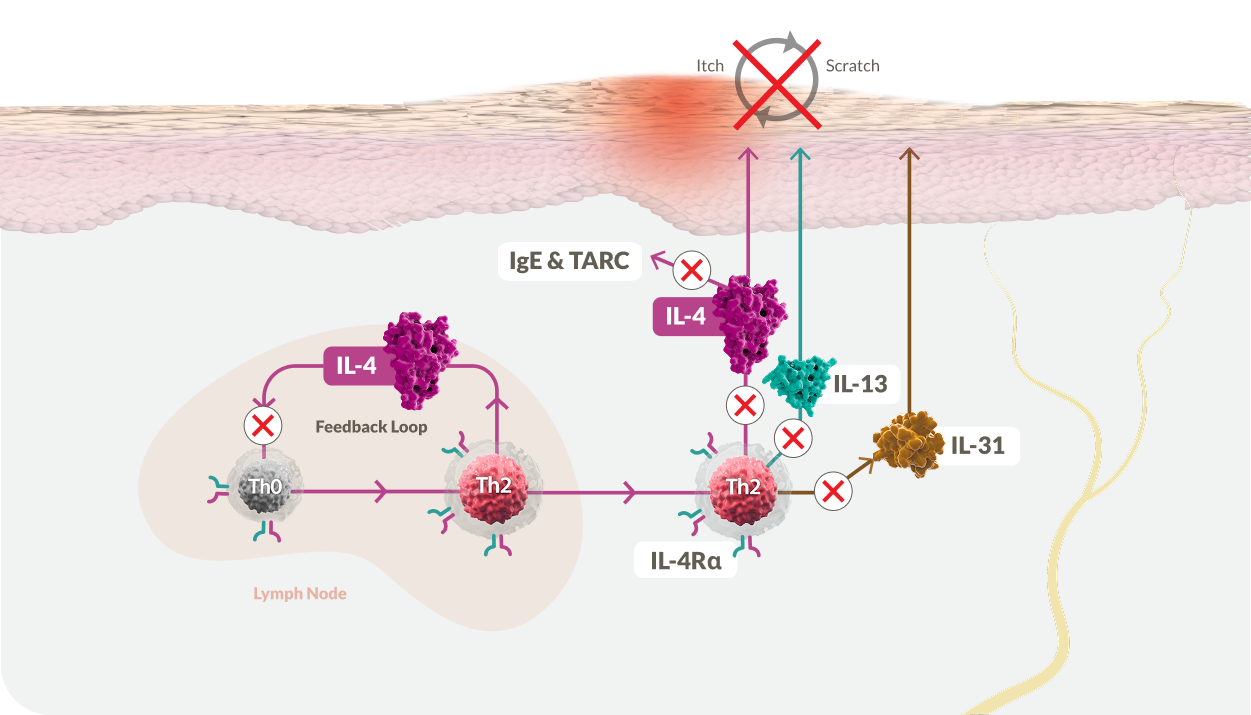
One target, dual action: by TARGETING IL-4Rα, only DUPIXENT blocks IL-4 and IL-13 signaling, and the type 2 inflammatory cascade that causes itch and skin damage13 |
DUPIXENT is the only biologic that inhibits IL-4 signaling, which initiates and perpetuates the type 2 cytokine cascade3,13,15,16
DUPIXENT directly inhibits IL-4Rα to impact AD and PN in at least 3 distinct ways3,9,13-17
REDUCES TYPE 2 INFLAMMATION |
HELPS CLEAR SKIN |
HELPS RELIEVE ITCH13 |
|
|
|
|
|
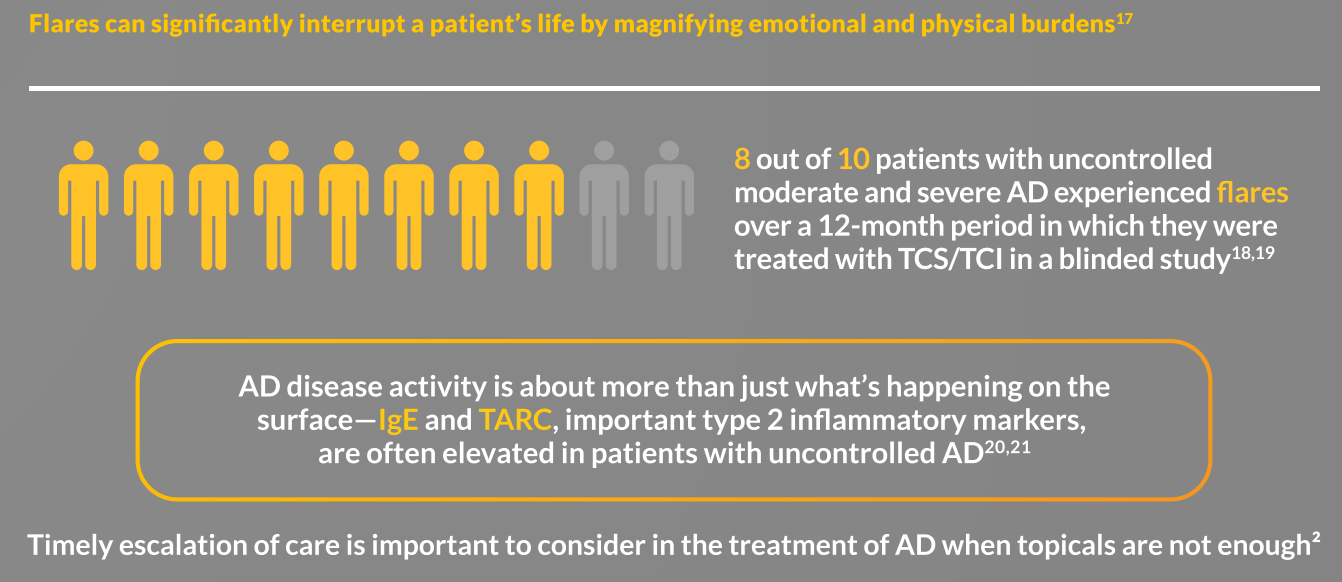
IgE and TARC (CCL17) play important roles in AD |
|
IgE |
TARC |
|
|


DUPIXENT may help lower IgE and TARC
- In a study of 780 patients (placebo groups n=287) with moderate-to-severe* AD treated with DUPIXENT, total IgE reduction range was -71% to -58% vs -21% to 28% with placebo (P<0.0001)18
- In the same study, TARC reduction range with DUPIXENT was -83% to -72% vs -15% to -2% with placebo (P<0.0001)18
*Dupixent is only approved for severe AD in children from 6 months to 11 years old
Footnotes
a Type 2 cytokines (eg, IL-4/IL-13/IL-31) may also be produced by other immune cells such as ILC2.32
Abbreviations
AD, atopic dermatitis; IL, interleukin; PN, prurigo nodularis; TARC, thymus and activation-regulated chemokine.
References
-
Williams KA et al. J Am Acad Dermatol. 2020;83(6):1567-1575.
-
Tsoi LC et al. J Allergy Clin Immunol. 2022;149(4):1329-1339.
-
Haddad E-B et al. Dermatol Ther (Heidelb). 2022;12(7):1501-1533.
-
Belzberg M et al. J Invest Dermatol. 2021;141(9):2208-2218.e14.
-
Palomares O et al. Immunol Rev. 2017;278(1):219-236.
-
Stott B et al. J Allergy Clin Immunol. 2013;132(2):446-454.e5.
-
Keegan AD et al. Fac Rev. 2021;10:71.
-
Beck LA et al. JID Innov. 2022;2(5):100131.
-
Weidinger S et al. Nat Rev Dis Primers. 2018;4(1):1.
-
Boesjes CM et al. Clin Exp Allergy. 2024;54(4):294-296.
-
Wirnsberger G et al. Eur J Immunol. 2006;36(7):1882-1891.
-
Kim BS et al. Presented at the Aspen Allergy Congress (AAC 2025); July 23-27, 2025; Aspen, CO, USA.
-
DUPIXENT Summary of Product Characteristics, 11/2025.
-
Silva-Filho JL et al. Biophys Rev. 2014;6(1):111-118.
-
Bieber T. Nat Rev Drug Discov. 2022;21(1):21-40.
-
Punnonen J et al. J Allergy Clin Immunol. 1997;100(6 Pt 1):792-801.
-
Romagnani S. J Allergy Clin Immunol. 2004;113(3):395-400.
-
Beck LA et al. J Allergy Clin Immunol. 2025;155(1):135-143.
-
Yosipovitch G et al. Nat Med. 2023;29(5):1180-1190.
-
Miake S et al. Int J Mol Sci. 2019;20(16):4053.
-
Edukulla R et al. J Biol Chem. 2015;290(21):13510-13520.
-
Oetjen LK et al. Cell. 2017;171(1):217-228.e13.
-
Nguyen JK et al. Arch Dermatol Res. 2020;312(2):81-92.
-
Serezani APM et al. J Allergy Clin Immunol. 2017;139(1):142-151.e5.
-
Silverberg JI, Kantor R. Dermatol Clin. 2017;35(3):327-334.
-
Mack MR et al. Front Mol Neurosci. 2023;16:1258823.
-
Pène J et al. Proc Natl Acad Sci USA. 1988;85(18):6880-6884.
-
Park CO et al. EBioMedicine. 2024;103:105121.
-
Wang F et al. Cell. 2021;184(2):422-440.e17.
-
Halling AS et al. J Allergy Clin Immunol. 2023;151(6):1550-1557.e6.
-
Catherine J, Roufosse F. Semin Immunopathol. 2021;43(3):439-458.
-
Bartemes KR, Kita H. J Allergy Clin Immunol. 2021;147(5):1531-1547.
Efficacy
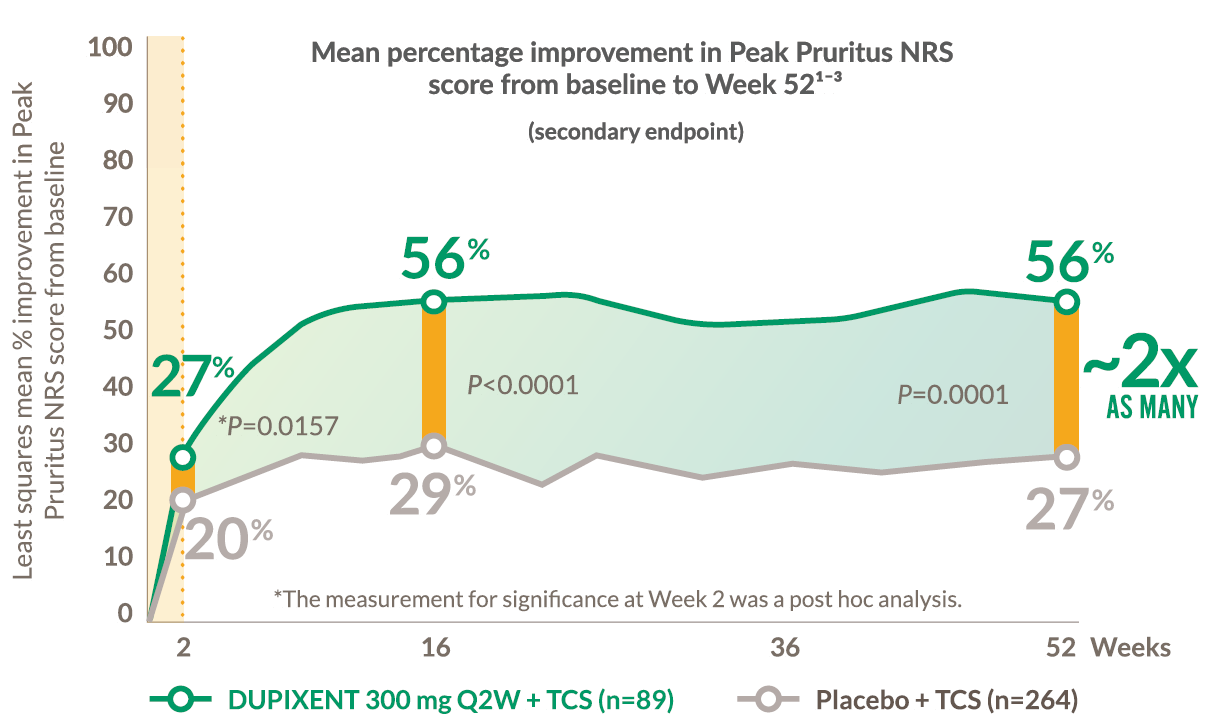
From the first dose, rapid and sustained symptom control and improved QoL were seen in adult patients with AD1-3
LIBERTY AD CHRONOS 18+ years
RAPID ITCH RELIEF SEEN AFTER THE FIRST DOSE WITH SIGNIFICANT AND SUSTAINED RELIEF AT WEEK 52
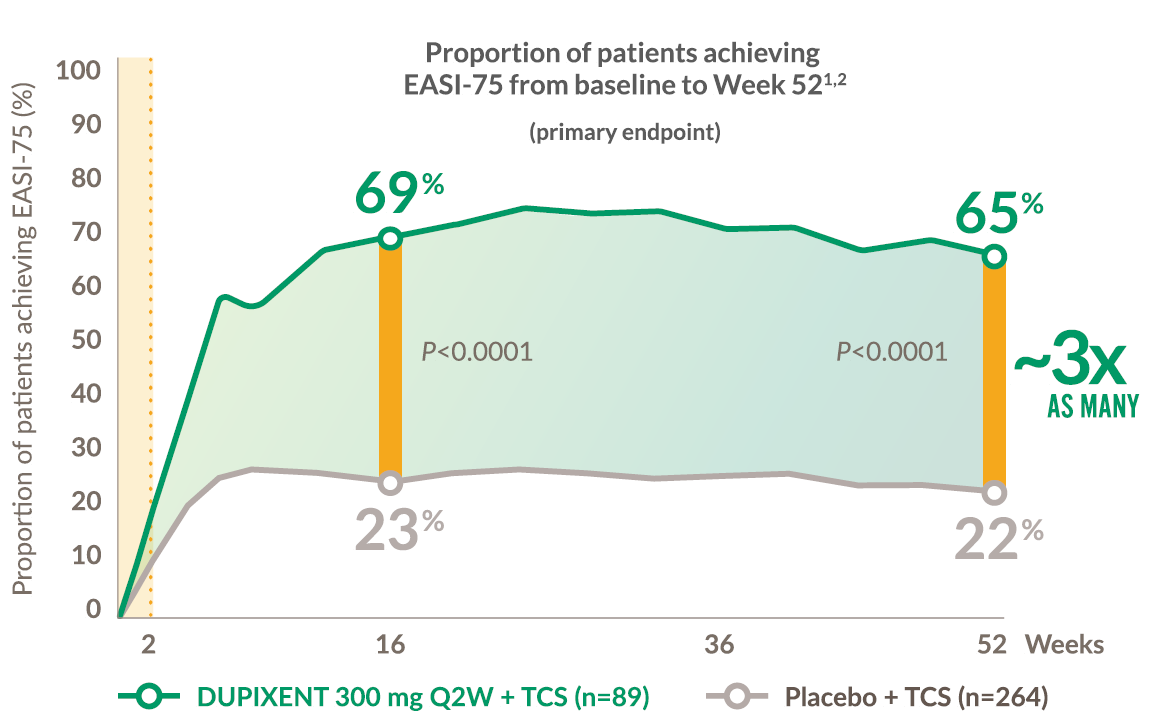
From the first dose, rapid and sustained symptom control and improved QoL were seen in adult patients with AD1-3
LIBERTY AD CHRONOS 18+ years
RAPID SKIN CLEARANCE FROM THE FIRST DOSE AND SUSTAINED AT WEEK 52
~50% of patients achieved EASI-90 on DUPIXENT + TCS compared to 16% with placebo + TCS at 52 weeks2,a
LIBERTY AD CHRONOS 18+ years
Improvement in lesion extent and severity (EASI) from baseline measured across body regions in adults at Week 52 (post hoc analysis)5

TRUNK
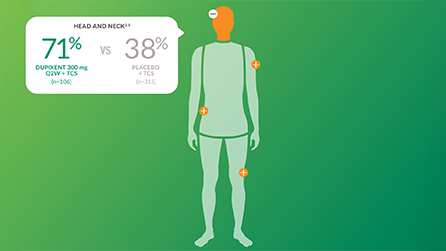
HEAD AND NECK
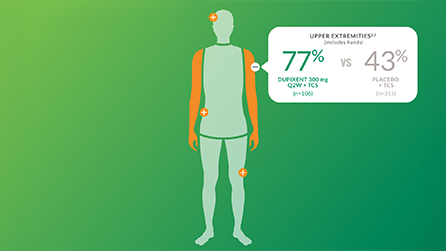
UPPER EXTREMITIES
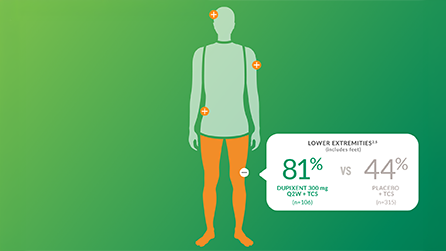
LOWER EXTREMITIES
From the first dose, rapid and sustained symptom control and improved QoL were seen in adult patients with AD1-3
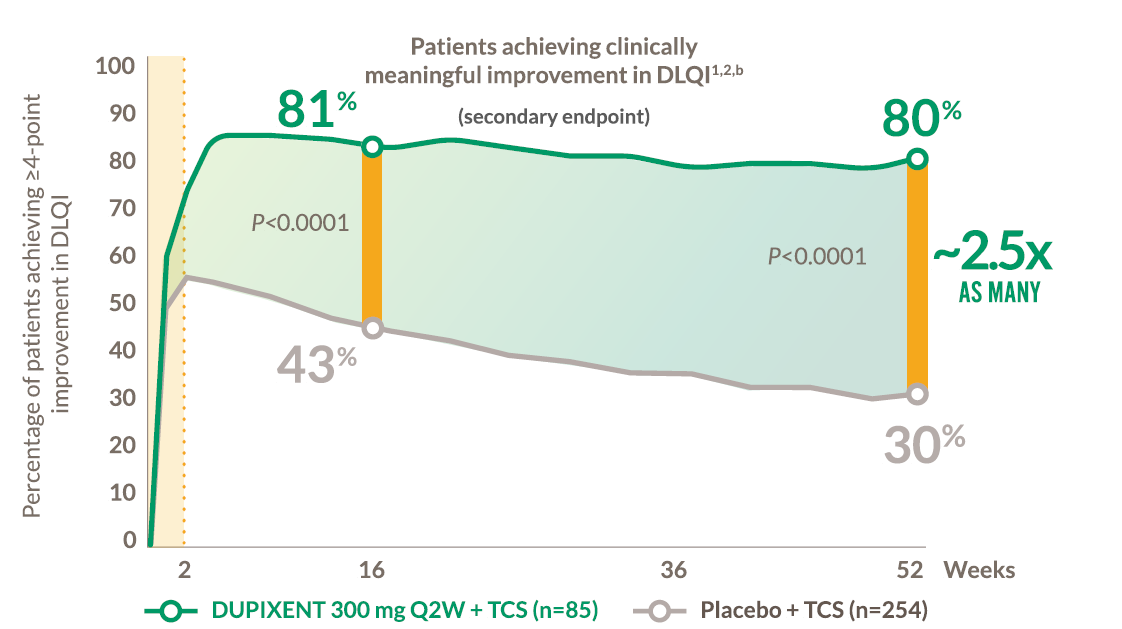
LIBERTY AD CHRONOS 18+ years
RAPID and sustained improvement in overall QoL at Week 52
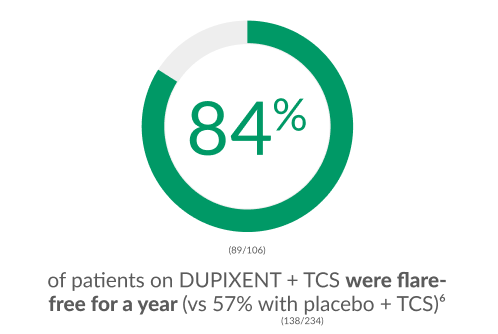
DUPIXENT PREVENTS FLARES6
IN A CLINICAL STUDY, THE MAJORITY OF PATIENTS TAKING DUPIXENT + TCS WERE FLARE-FREE FOR A YEAR
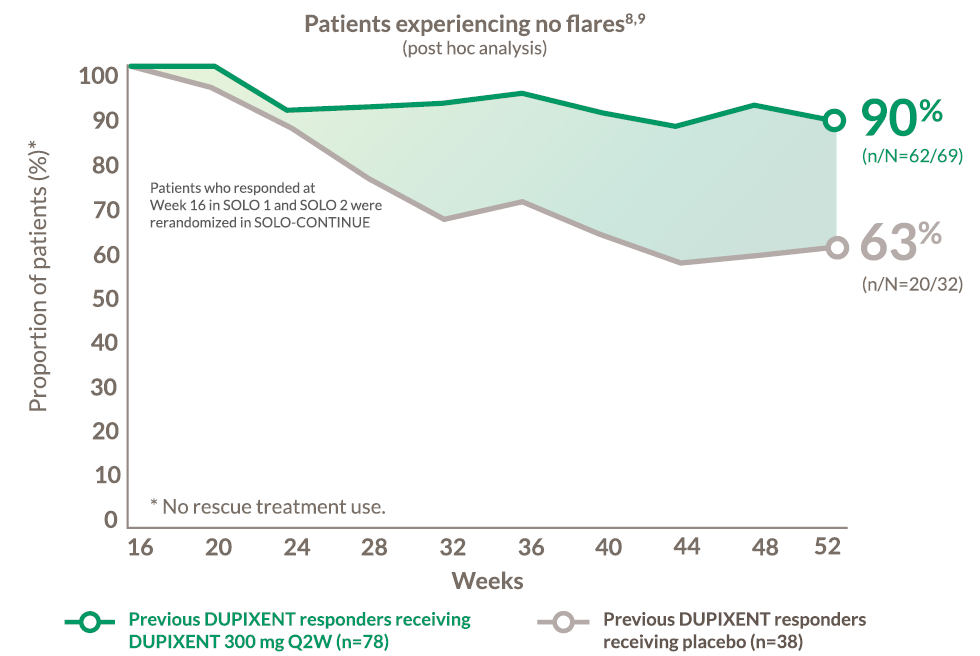
9 OF 10 DUPIXENT MONOTHERAPY RESPONDERS AT WEEK 16 EXPERIENCED NO FLARES AT 1 YEAR8,9
LIBERTY AD solo-continue 18+ years
DECREASE IN DAILY PEAK PRURITUS NRS FROM BASELINE OBSERVED IN ADULTS STARTING AS EARLY AS DAY 2 WITH DUPIXENT MONOTHERAPY7
Change in daily Peak Pruritus NRS from baseline in a post hoc analysis of pooled SOLO 1 and SOLO 2 trials (-4.5% with DUPIXENT [n=457] vs -0.6% with placebo [n=460])
SIGNIFICANT IMPROVEMENT IN ITCH, SKIN CLEARANCE, AND QoL IN HAND AND FOOT AD10
LIBERTY AD HAFT (12+)
HFE ITCH AND SKIN CLEARANCE |
Significant results in itch seen as early as Week 1, skin clearance at Week 2, and both sustained through Week 1610,c,d
RAPID ITCH IMPROVEMENT
Achieved ≥4-point improvement in Peak Pruritus NRS in hand and foot AD at Week 161,10

~4x AS MANY PATIENTS
with hand and foot AD taking DUPIXENT achieved itch improvement at Week 16 vs placebo1,10
(P<0.0001; secondary endpoint)
SUSTAINED SKIN CLEARANCE
Achieved IGAe 0 or 1 in AD at Week 161,10

~2x AS MANY PATIENTS
with hand and foot AD taking DUPIXENT achieved skin clearance at Week 16 vs placebo1,10
(P<0.01; primary endpoint)
HFE LESIONS |
Significant results in skin clearance seen as early as Week 2 and sustained through Week 1610,c,d
IMPROVEMENT IN HAND AND FOOT ATOPIC DERMATITIS LESIONS
Percent change from baseline at Week 16 in Hand Eczema
Severity Index (HECSI score, LS mean SE)10
(P<0.0001; primary endpoint)
HFE QoL |
Significant results in QoL seen as early as Week 2 and sustained through Week 1610,c,f
SLEEP QUALITY
Sleep Quality NRS: 1-point improvement with DUPIXENT vs 0 with placebo at Week 16
(P<0.05)10
HAND AND FOOT PAIN
Peak Pain NRS: 5-point improvement with DUPIXENT vs 2 with placebo at Week 16
(P<0.0001)10
QUALITY OF LIFE
QoLHEQ: 40-point improvement with DUPIXENT vs 16 with placebo at Week 16
(P<0.0001)10,g
Efficacy in adults11
LIBERTY AD OLE
DUPIXENT DELIVERED SUSTAINED IMPROVEMENT IN EASI OUT TO 4 YEARS IN THE REAL-WORLD CLINICAL SETTING11
In total, 127 patients received dupilumab 3000mg q2w and 61 patients received placebo
DUPISTAD, LIBERTY AD CHRONOS, and RELIEVE-AD as study indicators
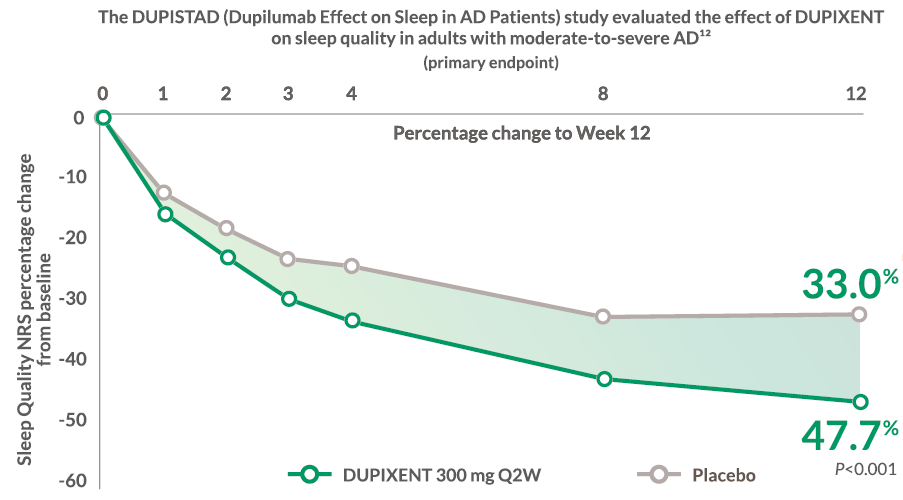
PATIENTS EXPERIENCED SLEEP IMPROVEMENT AT 3 MONTHS IN ONE TRIAL, AND MAINTAINED IT AT 4 YEARS IN ANOTHER11,12
In “Long-term efficacy and safety of dupilumab in adolescents with severe atopic dermatitis: a 3-year real-life study,” 95% of DUPIXENT patients had minimal or no sleep disturbance at 4 years11
LIBERTY AD SOLO 1, LIBERTY AD SOLO2, and RELIEVE-AD as study indicators
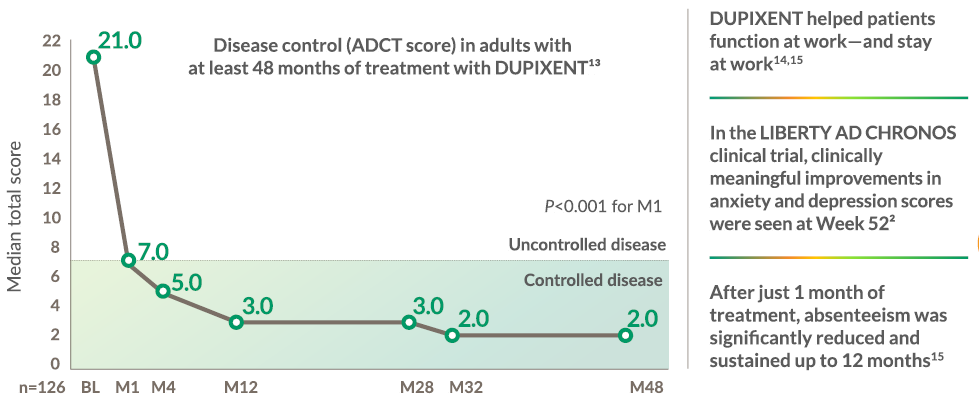
DUPIXENT delivered disease control for up to 4 years in the real-world clinical setting
DUPIXENT achieved disease control after 1 month and sustained up to 48 months (disease control defined as total ADCT score <7)13
LIBERTY AD CHRONOS
Continuous Dupixent treatment led to LONG-LASTING DISEASE CONTROL IN THE REAL-WORLD CLINICAL SETTING
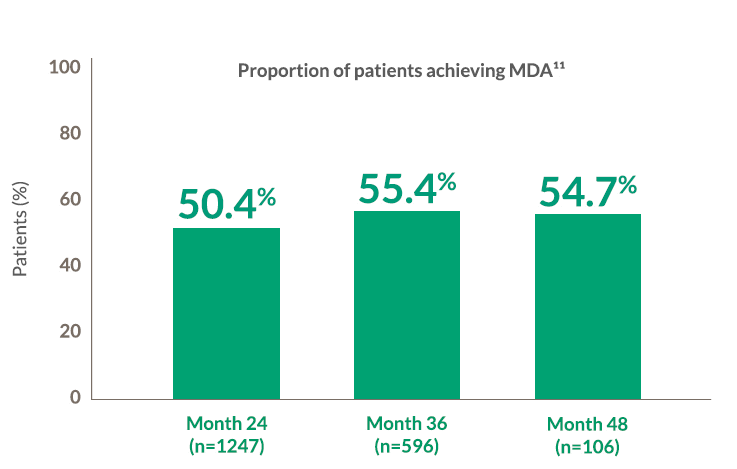
More than half of patients maintained Minimal Disease Activity (MDA) at 4 years on treatment with DUPIXENT11
MDA target criteria were defined as: EASI-90, Itch NRS score ≤1, Sleep NRS score ≤1, and DLQI ≤111
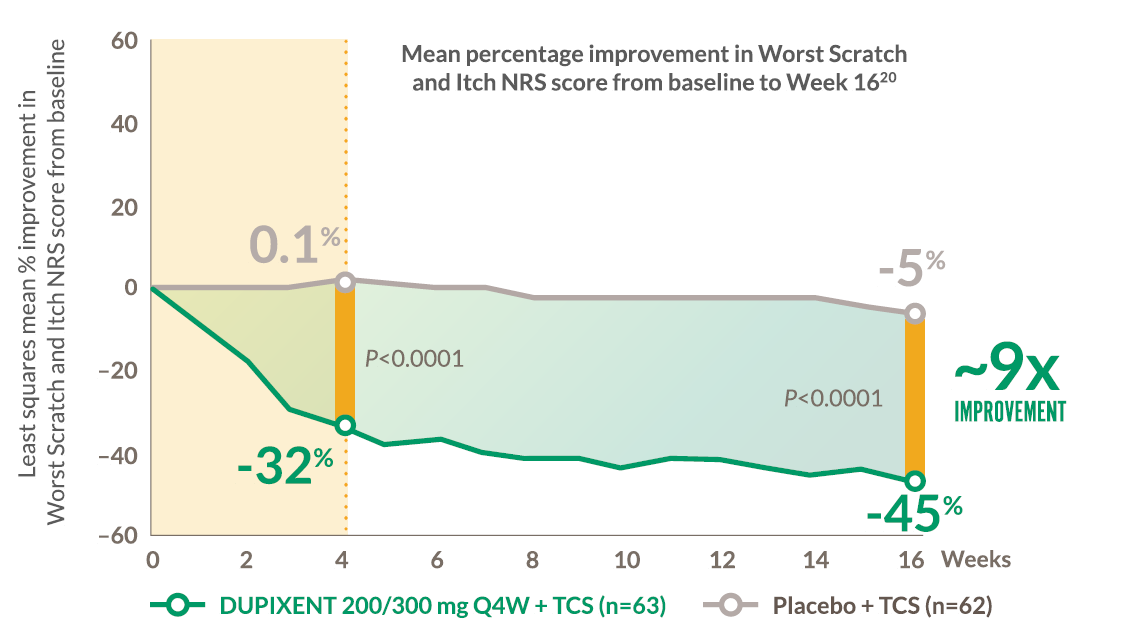
CHILDREN AGED 6 MONTHS TO 5 YEARS WITH SEVERE AD HAD RAPID CONTROL AFTER THE FIRST DOSE AND SUSTAINED UP TO 16 WEEKS20
Liberty AD PRESCHOOL
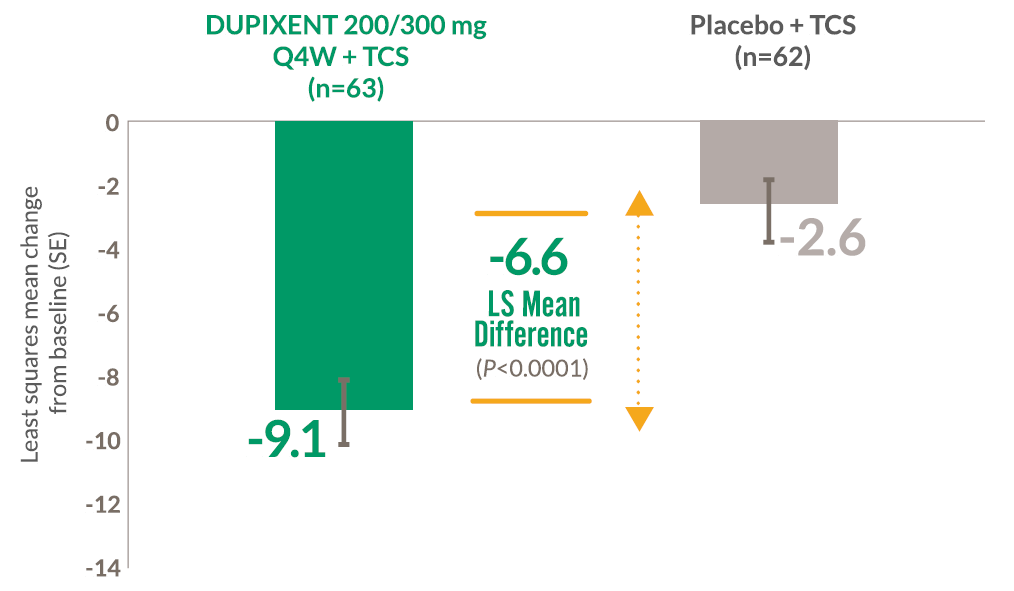
Significant improvement in Worst Scratch and Itch NRS score at Week 16
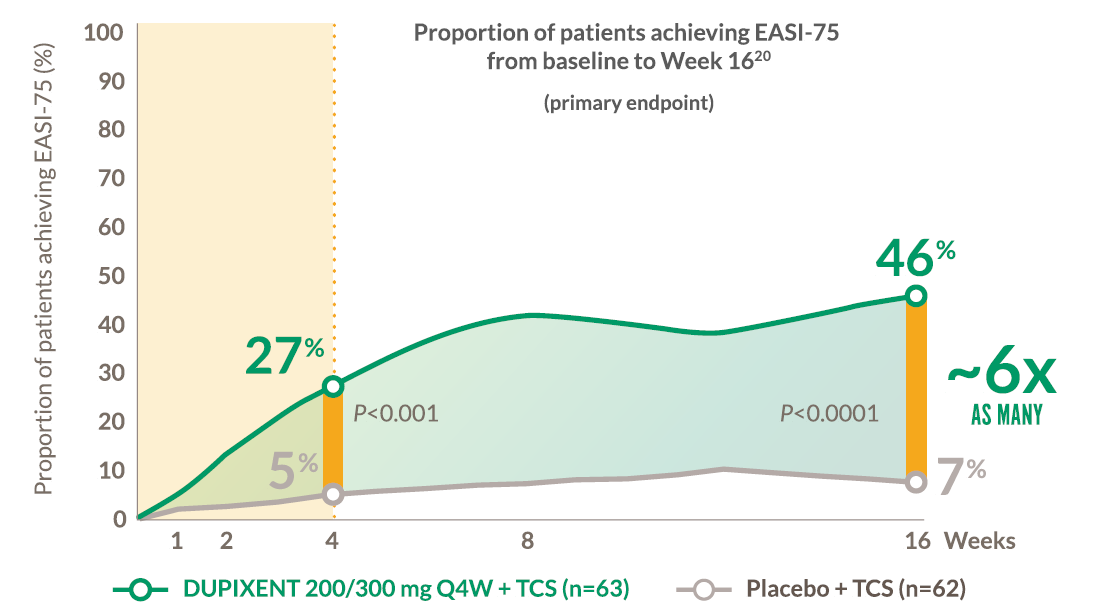
LIBERTY AD PRESCHOOL
Rapid and sustained skin clearance at Week 16
LIBERTY AD PRESCHOOL
Significant improvement in CDLQI at Week 16
Mean change from baseline in CDLQIl at Week 1620
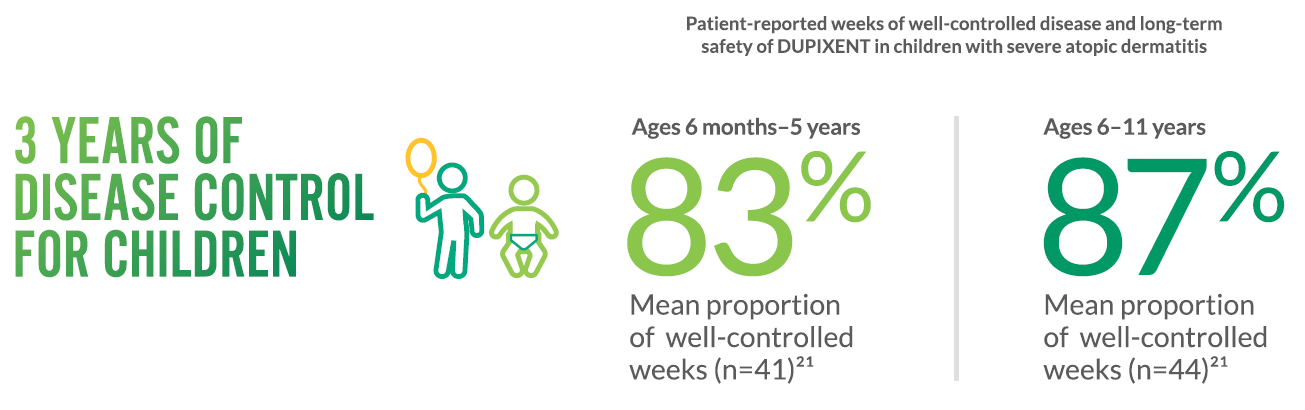
Efficacy in children21
With Dupixent, people with severe AD, showed high proportions of well-controlled weeks at 3 years in an open-label extension study: LIBERTY AD PED-OLE
VISIBLE RESULTS

This adult patient was an actual patient treated with DUPIXENT. Not a clinical trial patient. Scoring was designated by the treating physician.
Because this was a real-world patient, other factors may have influenced their treatment results. Individual results may vary.
Images used with informed patient consent. Sanofi, US Photo Project 2019 B04 (RWD)

Actual 12-year-old patient in the phase 3 adolescent DUPIXENT trial (AD-1526). Patient had a baseline IGA of 4 and EASI of 31. Individual results may vary.
- This adolescent patient did not meet the primary endpoint in the clinical trial based on their IGA score at Week 16
A clinical responder was defined as a patient achieving IGA 0 or 1 and at least a 2-point improvement from baseline.1 Images used with informed patient consent.

Actual 6-year-old patient in a phase 3 DUPIXENT trial (AD-1652) in children (6-11 years of age). Patient was prescribed concomitant TCS based on the clinical trial program.
This patient was considered a clinical responder. Individual results may vary.
A clinical responder was defined as a patient achieving IGA 0 or 1 and at least a 2-point improvement from baseline.1 Images used with informed patient consent.

Actual 4-year-old patient in a phase 3 DUPIXENT trial (AD-1539) in infants to young children (aged 6 months to <6 years). Patient was prescribed concomitant low-potency
TCS based on the clinical trial protocol. This patient was considered a clinical responder. Individual results may vary.
A clinical responder was defined as a patient achieving IGA 0 or 1 and at least a 2-point improvement from baseline.1 Images used with informed patient consent.
STUDY DESIGNS
LIBERTY AD CHRONOS was a randomized, double-blind, placebo-controlled trial in adults with moderate-to-severe atopic dermatitis (N=740), randomized to DUPIXENT 300 mg Q2W + TCS (n=106) or placebo + TCS (n=315) for 52 weeks. Coprimary endpoints were the proportion of patients achieving EASI-75, and an IGA score of 0 or 1 with a reduction from baseline of ≥2 points at Week 16. The most common comorbid type 2 immune diseases at baseline were allergies (other than food allergy), allergic rhinitis, and asthma.2
LIBERTY AD SOLO 1 (N=671), and LIBERTY AD SOLO 2 (N=708) were two independent, randomized, double-blind, placebo-controlled, parallel-group trials of identical design in adults with moderate-to-severe atopic dermatitis, randomized to DUPIXENT 300 mg or placebo weekly or the same dose of dupilumab every other week alternating with placebo for 16 weeks. The coprimary endpoints were proportion of patients with EASI-75, and proportion of patients with both IGA 0 to 1 and a reduction from baseline of ≥2 points, at Week 16.26
RELIEVE-AD was a prospective, longitudinal survey on disease control and treatment satisfaction among adult patients in the US with atopic dermatitis.27
In the BALISTAD study a total of 52 subjects were enrolled, of which 26 participants were each enrolled into the AD cohort and the healthy volunteers (HV) cohort. AD subjects received dupilumab at Day 1 and Weeks 2, 4, 6, 8, 10, 12, and 14 subcutaneously at a loading dose of 600 mg with subsequent doses of 300 mg. The doses were decreased to 400 mg loading dose and 200 mg subsequent doses if subject’s weight was below 60 kg. HV subjects were age and gender-matched with AD subjects and did not receive any treatment.17
LIBERTY AD HAFT was a randomized phase 3 trial in adults and adolescents with moderate-to-severe hand and foot atopic dermatitis inadequately controlled with topical prescription therapies. Patients were given dupilumab monotherapy or placebo. Adults and adolescents with a body weight ≥60 kg who received DUPIXENT were given 300 mg Q2W after a 600 mg loading dose. Adolescents with a body weight <60 kg who received DUPIXENT were given 200 mg after a 400 mg loading dose. Adult patients had chronic hand and/or foot eczema for at least 3 years and adolescents for 1 year. At baseline, 72.2% had an IGA of hand and foot score of 3 (moderate), and 27.8% had an IGA of hand and foot score of 4 (severe), and weekly averaged Peak Pruritus NRS was 7.1 on a scale of 0 to 10.10
LIBERTY AD PRESCHOOL was a two-part phase 2/3 trial. The phase 3 randomized, double-blind, placebo-controlled 16-week trial (Part B) was in children aged 6 months to 5 years with uncontrolled moderate-to-severe atopic dermatitis (N=162), randomized to DUPIXENT 200 mg (for children weighing ≥5 to <15 kg) or 300 mg (for children weighing ≥15 to <30 kg) Q4W (n=83) or placebo (n=79), plus low-potency TCS. Coprimary endpoints were the proportion of patients achieving EASl-75 and an IGA score of 0 or 1 at Week 16.1,28
LIBERTY AD PEDS was a randomized, double-blind, placebo-controlled trial in children aged 6-11 years with severe atopic dermatitis (N=367) whose disease was inadequately controlled by topical treatment, randomized to DUPIXENT 300 mg Q4W + TCS, 100/200 mg Q2W + TCS, or placebo + TCS for 16 weeks. Coprimary endpoints were the proportion of patients achieving EASl-75 and an IGA score of 0 or 1 with a reduction from baseline of ≥2 points at Week 16.1,29
LIBERTY AD ADOL was a randomized, double-blind, placebo-controlled, parallel-group study in adolescents with moderate-to-severe atopic dermatitis (N=251) whose disease was inadequately controlled by topical treatment, randomized to DUPIXENT 200/300 mg Q2W or placebo for 16 weeks. Coprimary endpoints were the proportion of patients achieving EASI-75 and an IGA score of 0 or 1 with a reduction from baseline of ≥2 points at Week 16.1,30
AD-1412 was a global, multicenter, phase 2a, open-label, ascending dose, cohort study in children aged ≥6 to <18 years with atopic dermatitis. In the phase 2a study, patients received DUPIXENT 2 mg/kg or 4 mg/kg once, followed by 8 weeks of pharmacokinetic sampling, thereafter receiving the same dose QW for 4 weeks with 8-week safety follow-up. Primary endpoint was characterization of the pharmacokinetic profile of DUPIXENT. Secondary endpoints included incidence of AEs and percentage change from baseline in EASI and PP-NRS score.31
LIBERTY AD PED-OLE is an ongoing phase 3, OLE trial in pediatric patients aged ≥6 months to <18 years with moderate- to-severe atopic dermatitis who participated in DUPIXENT parent trials. Patients received DUPIXENT 300 mg Q4W. If patients did not achieve an IGA score of 0/1 within at least 16 weeks from start of treatment with 300 mg Q4W, they could be uptitrated to 200 mg Q2W (for body weight <60 kg) or 300 mg Q2W (for body weight ≥60 kg) at Week 16 or prior to Week 16 at the discretion of the treating physician. The study consisted of a screening period (Day -28 to Day -1) between exit from the parent study and entry into the OLE study, a treatment period that lasts until regulatory approval of the product for the age group of the patients in their geographical region, and a 12-week follow-up period. Primary endpoints were incidence and rate of TEAEs. Secondary outcomes included incidence and rate of SAEs, TEAEs of special interest, and efficacy and assessment of QoL up to Week 52.31-33
A retrospective study conducted at a single tertiary care center in Italy, which included 126 patients with severe AD who were treated with DUPIXENT for at least 48 months at standard doses (600 mg at the baseline, then 300 mg every other week). Patients who had discontinued therapy even temporarily for more than one month were excluded. The aim of the study was to evaluate the trend of patient-reported outcomes (PROs) during DUPIXENT treatment over 4 years and their correlation with clinical response. Scores for EASI and PROs, Pruritus NRS, Sleep NRS, POEM, ADCT, and DLQI were collected at baseline, after one month of treatment, after 4 months of treatment, and then every 4 months until 48 months of treatment.13
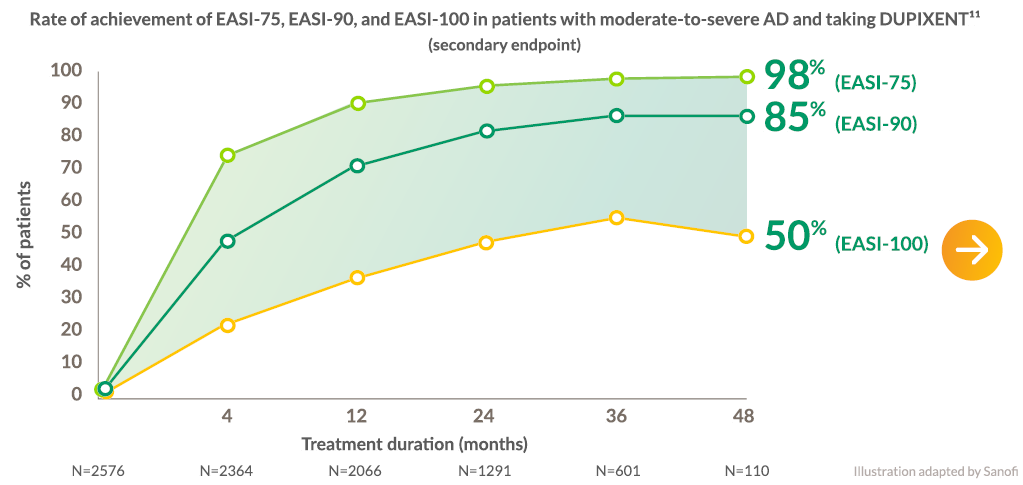
A multicenter, retrospective, dynamic cohort study conducted to assess the long-term effectiveness and safety of DUPIXENT up to 48 months in patients with moderate-to-severe AD in a real-world setting. 2576 patients were included from 24 Italian dermatological centers from June 2018 to July 2022, of whom 2066 and 110 had data available for analysis at 12 and 48 months respectively. DUPIXENT was prescribed according to recommendations of the Italian Drug Agency (AIFA), and patients were allowed to use rescue medications (including topical corticosteroids or topical calcineurin inhibitors) as prescribed by their treating physicians once or twice a day for AD control in critical areas. EASI scores and PROs, including weekly average NRS for pruritus and sleep disturbances as well as DLQI, recorded at baseline and at 4, 12, 24, 36, and 48 months of follow-up were extracted. Primary endpoint was to identify predictors of MDA achievement at available timepoints, and secondary endpoints included achievement of EASI-75, EASI-90, and EASI-100, as well as PROs reductions at available timepoints.11
LIBERTY AD OLE was a multicenter, open-label trial in adults with moderate-to-severe atopic dermatitis (N=2677). At enrollment, patients initiated a regimen of subcutaneous dupilumab, 200 mg, weekly (400-mg loading dose). The regimen was amended in June 2014 to dupilumab, 300 mg, weekly (600-mg loading dose) based on a dose-ranging study and again in November 2019 to dupilumab, 300 mg, every 2 weeks to align with the regulatory regimen approvals. The primary outcome was incidence and rate of TEAEs. Key secondary outcomes included incidence and rate of serious TEAEs, percentage of patients with an IGA score of 0/1, and percentage of patients with ≥75% improvement in EASI from baseline (EASI-75).34
A retrospective study of 2576 patients with moderate-to-severe AD who were treated with dupilumab as standard care at 24 Italian dermatological centers from June 2018 to July 2022. The primary endpoint was to identify predictors of MDA achievement at available timepoints of 4, 12, 24, 36, and 48 months. Secondary endpoints included achievement of EASI-75, EASI-90, and EASI-100, as well as PRO reductions.11
BioDay is an ongoing, prospective, multicenter observational study of 1286 patients of all ages with a median (IQR) age of 38 (26-54) years from the BioDay registry (4 academic and 10 nonacademic Dutch hospitals), all treated with dupilumab between October 2017 and December 2022. Adults (≥18 years) received a loading dose of subcutaneous dupilumab, 600 mg, at baseline, followed by 300 mg every other week. Primary clinical effectiveness outcomes included EASI, IGA, and NRS for pruritus in the past week.35
In DUPISTAD (Dupilumab Effect on Sleep in AD Patients), a phase 4, randomized, double-blind, placebo-controlled study, the primary endpoint was the percentage change in sleep quality from baseline to Week 12, assessed using a novel NRS. This study specifically focused on the impact of dupilumab on sleep in adults with moderate-to-severe atopic dermatitis. A total of 188 patients were enrolled in the study. 127 patients received DUPIXENT, while 61 patients received placebo. Patients were randomized in a 2:1 ratio (DUPIXENT:placebo). Participants randomized to the active treatment arm received DUPIXENT 300 mg administered as a subcutaneous injection Q2W. This typically followed a loading dose of 600 mg on Day 1 for the DUPIXENT group. Concomitant topical corticosteroids were permitted. After the initial 12-week, double-blind, placebo-controlled phase, all patients entered an open-label phase and received DUPIXENT 300 mg Q2W for a further 12 weeks.12
LIBERTY AD SOLO-CONTINUE was a randomized, double-blind, phase 3 clinical trial conducted from March 25, 2015, to October 18, 2016 at 185 sites in North America, Europe, Asia, and Japan. Patients with moderate-to-severe AD who received DUPIXENT treatment and achieved an Investigator’s Global Assessment score of 0 or 1 or 75% improvement in Eczema Area and Severity Index score (EASI-75) at Week 16 in 2 previous DUPIXENT monotherapy trials (LIBERTY AD SOLO 1 and 2) were rerandomized in SOLO-CONTINUE. After completing SOLO-CONTINUE, patients were followed up for up to 12 weeks or enrolled in an open-label extension. Data were analyzed from December 5 to 12, 2016.9
Footnotes
a P<0.0001.1
b Based on ≥4-point improvement in DLQI.2
c BSA of each hand=1%.36
d Improvements in itch at Week 1 and skin clearance at Week 2 were nominally significant.10
e Hand and foot AD.
f Improvement in QoL at Week 2 was nominally significant.10
g QoL improvement was measured by the Quality of Life in Hand Eczema Questionnaire, a disease-specific instrument that consists of 30 items that are grouped by 4 domains of health-related quality of life: symptoms, emotions, functioning, and treatment and prevention. QoLHEQ single scores (κ-coefficient of agreement, 0.431) were not at all, 0–10; slightly, 11–39; moderately, 40–61; strongly, 62–86; and very strongly, ≥87.37
h A total of 52 subjects were enrolled, of which 26 participants were each enrolled into the AD cohort and the healthy volunteers (HV) cohort. AD subjects received dupilumab at Day 1 and Weeks 2, 4, 6, 8, 10, 12, and 14 subcutaneously at a loading dose of 600 mg with subsequent doses of 300 mg. The doses were decreased to 400 mg loading dose and 200 mg subsequent doses if subject’s weight was below 60 kg. HV subjects were age and gender-matched with AD subjects and did not receive any treatment.17
i Longitudinal TEWL AUC10 data (the sum of TEWL measurements collected at the surface of the skin and after 5 and 10 skin tape strips represented as median with 95% confidence interval by skin type [lesional, nonlesional, and healthy skin]).17
j At baseline, the median TEWL AUC10 in AD lesional skin was significantly different from that of healthy volunteers (P<0.0001).17
k At Week 16, the adjusted mean (95% CI) TEWL AUC10 in AD lesional skin was not significantly different from that of healthy volunteers (ANCOVA; P=0.261).17
l CDLQI was measured in patients ≥4 years of age.20
Abbreviations
AD, atopic dermatitis; ADCT, Atopic Dermatitis Control Tool; AE, adverse event; ANCOVA, analysis of covariance; AUC, area under the curve; BSA, body surface area; CDLQI, Children’s Dermatology Life Quality Index; DLQI, Dermatology Life Quality Index; EASI, Eczema Area and Severity Index; HFE, hand-foot eczema; HR, hazard ratio; IGA, Investigator’s Global Assessment; LS, least squares; M, month; NRS, Numeric Rating Scale; OLE, open-label extension; POEM, Patient Oriented Eczema Measure; QW, once weekly; Q2W, once every 2 weeks; Q4W, once every 4 weeks; QoL, quality of life; QoLHEQ, Quality of Life in Hand Eczema Questionnaire; SAE, serious adverse event; TCI, topical calcineurin inhibitors; TCS, topical corticosteroids; TEAE, treatment-emergent adverse event.
References
1. DUPIXENT Summary of Product Characteristics, 11/2025.
2. Blauvelt A et al. Lancet 2017;389(10086):2287-2303.
3. Blauvelt A et al. Lancet 2017;389(10086):2287-2303 [suppl.].
5. Blauvelt A et al. Br J Dermatol 2019;181(1):196-197.
6. Merola JF et al. J Am Acad Dermatol 2021;84(2):495-497.
7. Thaçi D et al. J Dermatol Sci 2019;94(2):266-275.
8. Simpson EL et al. Poster presented at the 14th Georg Rajka International Symposium on Atopic Dermatitis (ISAD 2024); October 24-26, 2024; Doha, Qatar.
9. Worm M et al. JAMA Dermatol 2020;156(2):131-143.
10. Simpson EL et al. J Am Acad Dermatol 2024;90(6):1190-1199.
11. Ferrucci S et al. Clin Exp Dermatol 2024;49(12):1561-1572.
12. Merola JF et al. Br J Dermatol 2023;189(6):685-694.
13. Barei F et al. Pharmaceuticals 2024;17(1):117.
14. Bosma AL et al. J Dermatol 2021;48(9):1305-1314.
15. Ariëns LFM et al. Acta Derm Venereol 2021;101:adv00573.
16. Simpson EL et al. J Allergy Clin Immunol 2023;152(5):1179-1195.
17. Berdyshev E et al. Allergy 2022;77(11):3388-3397.
18. Blauvelt A et al. Adv Ther 2023;40(1):367-380.
19. Lin TL et al. Ann Allergy Asthma Immunol 2025;134(3):333-340.e6.
20. Paller AS et al. Adv Ther 2024;41(3):1046-1061.
21. Paller AS et al. Poster presented at the 24th European Society for Pediatric Dermatology (ESPD) Congress; May 29-31, 2025; Brussels, Belgium.
24. Tsai SYC et al. Allergy 2024;79(10):2748-2758.
25. Zirpel H et al. J Dermatolog Treat 2024;35(1):2421429.
26. Simpson EL et al. N Engl J Med 2016;375(24):2335-2348.
27. Kimball AB et al. Dermatol Ther (Heidelb) 2023;13(9):2107-2120.
28. Paller AS et al. Lancet 2022;400(10356):908-919.
29. Paller AS et al. J Am Acad Dermatol 2020;83(5):1282-1293.
30. Simpson EL et al. JAMA Dermatol 2020;156(1):44-56.
31. Cork MJ et al. Br J Dermatol 2020;182(1):85-96.
32. Blauvelt A et al. Am J Clin Dermatol 2022;23(3):365-383.
33. Cork MJ et al. Dermatol Ther (Heidelb) 2023;13(11):2697-2719.
34. Beck LA et al. Am J Clin Dermatol 2020;21(4):567-577.
35. Boesjes CM et al. JAMA Dermatol 2024;160(10):1044-1055.
36. Minnesota Department of Health. Determining Total Body Surface Area. April 2019. Accessed June 13, 2025. https://www.health.state.mn.us/communities/ep/surge/burn/tbsa.pdf
37. Oosterhaven JAF et al. J Invest Dermatol 2020;140(4):785-790.
Safety
DUPIXENT HAS DEMONSTRATED LONG-TERM SAFETY AND TOLERABILITY1
In adults with AD, the safety and tolerability profile of DUPIXENT has been studied for 5 years in an open-label extension study1
- The safety and tolerability profile of DUPIXENT was shown to be generally consistent with 52-week data1
- Skin infection risk with DUPIXENT did not increase1
DUPIXENT has demonstrated a consistent safety profile across a broad range of indications, including from infants to adults in AD1
Open-label extension, final data set2
DUPIXENT 300 mg QWa (N=2677)
Number of events |
Patients with ≥1 event, n (%) |
nP/100PY |
|
| TEAEs | 14,717 | 2276 (85.0) | 166.0 |
| Severe TEAEs | 391 | 269 (10.0) | 5.0 |
| Serious TEAEs | 388 | 283 (10.6) | 5.2 |
| Serious TEAEs related to treatmentb | 38 | 33 (1.2) | 0.6 |
| TEAEs leading to study drug discontinuation | 122 | 101 (3.8) | 1.7 |
IMPORTANT CONSIDERATIONS
Not metabolized through the liver or excreted through the kidneys1

No requirement for initial lab testing or ongoing lab monitoring1

No known drug-to-drug interactions1
Please see DUPIXENT Summary of Product Characteristics for additional safety information.
Consistent safety across indications1
Adverse reactions for DUPIXENT in clinical studies1 |
||
System organ class |
Frequency |
Adverse reaction |
| Infections and infestations | Common |
Conjunctivitisc Oral herpesc |
| Blood and lymphatic system
disorders |
Common | Eosinophilia |
| Immune system disorders |
Uncommon Rare |
Angioedemad Anaphylactic reactions, serum sickness reactions, serum sickness like reactions |
| Eye disorders |
Common Uncommon Rare |
Conjunctivitis allergicc Keratitis,c,d blepharitis,c,e eye pruritus,c,e dry eyec,e
|
| Skin and subcutaneous tissue
disorders |
Uncommon | Facial rashd |
| Musculoskeletal and connective
tissue disorders |
Common | Arthralgiad |
| General disorders and
administration site conditions |
Common | Injection site reactions (includes erythema, edema, pruritus, pain, swelling, and bruising) |
- If a systemic hypersensitivity reaction (immediate or delayed) occurs, DUPIXENT should be discontinued immediately and appropriate therapy initiated1
- Patients who develop conjunctivitis that does not resolve following standard treatment should undergo ophthalmological examination1
- Patients with comorbid asthma should not adjust or stop their asthma treatments without consulting their physicians. Monitor patients with comorbid asthma carefully following discontinuation of DUPIXENT1
- Most patients experiencing conjunctivitis recovered or were recovering during the treatment period1
- Treat any pre-existing helminth infections prior to initiating treatment with DUPIXENT. If patients become infected while receiving treatment with DUPIXENT and do not respond to anti-helminth treatment, discontinue treatment with DUPIXENT until the infection resolves1
Footnotes
a Includes the 226 patients who switched from 300 mg QW to 300 mg Q2W in Amendment 9 (Nov. 2019).2
b All serious treatment-related TEAEs were observed in 1 or 2 patients each. MedDRA-preferred terms reported in 2 patients each were gastroenteritis, influenza, pneumonia, urosepsis, and Hodgkin disease.2
c Eye disorders and oral herpes occurred predominately in atopic dermatitis studies.1
d From postmarketing reporting.1
e The frequencies for eye pruritus, blepharitis, and dry eye were common, and ulcerative keratitis was uncommon in atopic dermatitis studies.1
Abbreviations
AD, atopic dermatitis; MedDRA, Medical Dictionary for Regulatory Activities; QW, once weekly; Q2W, once every 2 weeks; TEAE, treatment-emergent adverse event.
References
-
DUPIXENT Summary of Product Characteristics, 11/2025.
-
Beck LA et al. JAMA Dermatol 2024;160(8):805-812.
Dosing
DOSING IN ATOPIC DERMATITIS1,a

Self-inject with confidence (patients 2+ years of age)*
Patients can self-inject using the pre-filled auto-injection pen.1,2
Provide proper training to patients and/or caregivers on the preparation and administration of DUPIXENT prior to use.
*In children 12 years of age and older, it is recommended that dupilumab is administered by or under supervision of an adult. In children 6 months to less than 12 years of age, dupilumab should be given by a caregiver.
A fast and simple experience
The DUPIXENT pre-filled auto-injection pen is designed for patients
- No reconstitution needed
- Buttonless activation
- Clear visual feedback
- Injection takes seconds
- 14-day out-of-fridge storage at room temperature
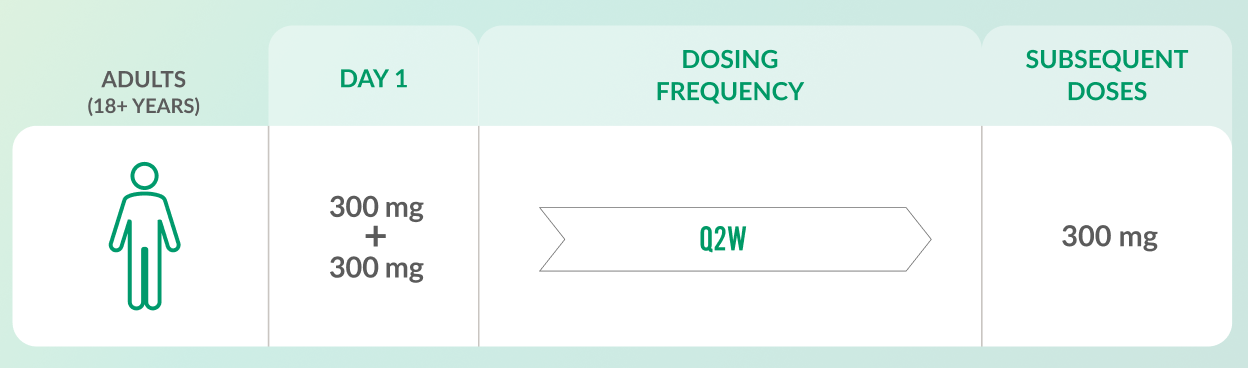
ADULTS (18+ YEARS)
- DUPIXENT provides you and your patients with a pre-filled syringe or the choice of an auto-injection pen (patients 2+ years)1
- Provide proper training to patients and/or caregivers on the preparation and administration of DUPIXENT prior to use.
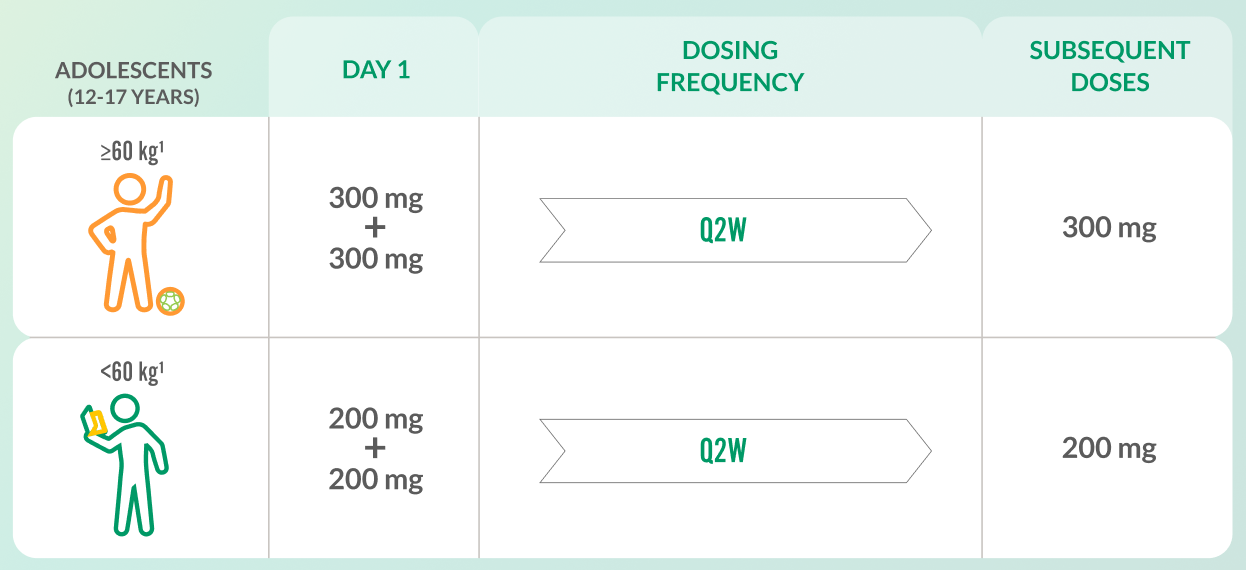
ADOLESCENTS (12-17 YEARS)
- DUPIXENT provides you and your patients with a pre-filled syringe or the choice of an auto-injection pen (patients 2+ years)1
- Provide proper training to patients and/or caregivers on the preparation and administration of DUPIXENT prior to use.
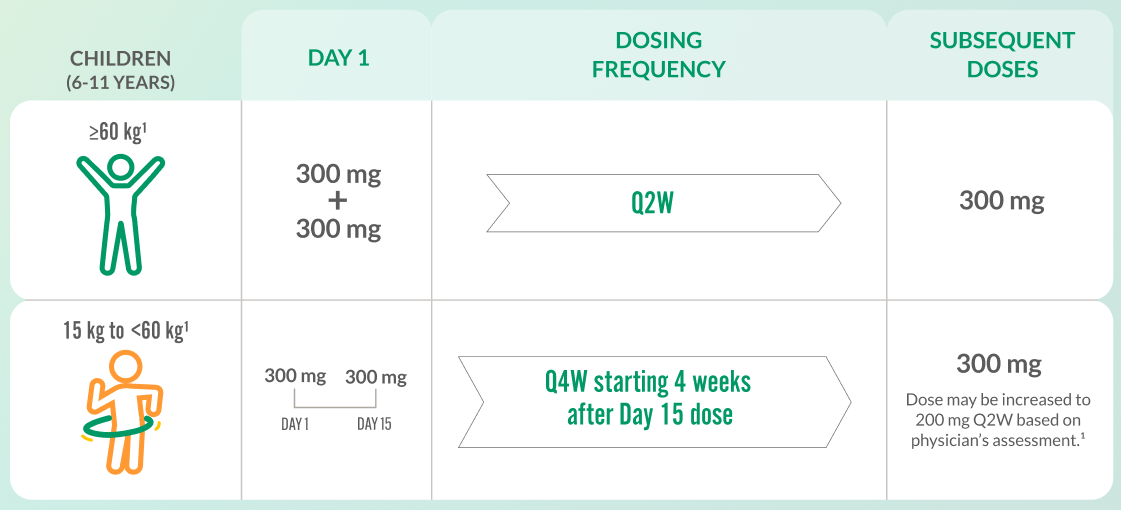
CHILDREN (6-11 YEARS)
- DUPIXENT provides you and your patients with a pre-filled syringe or the choice of an auto-injection pen (patients 2+ years)1
- Provide proper training to patients and/or caregivers on the preparation and administration of DUPIXENT prior to use.
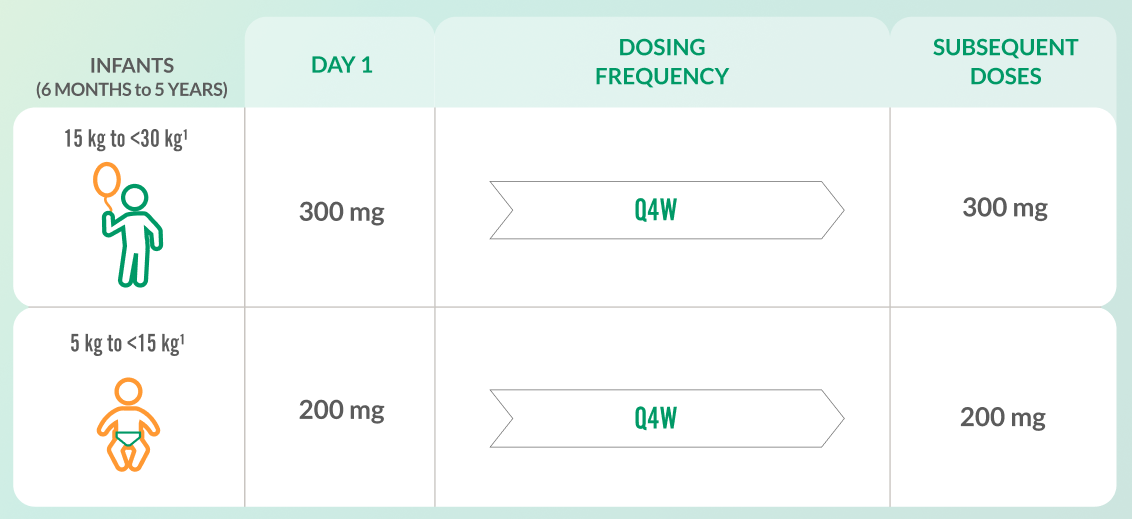
INFANTS (6 MONTHS TO 5 YEARS)
- DUPIXENT provides you and your patients with a pre-filled syringe or the choice of an auto-injection pen (patients 2+ years)1
- Provide proper training to patients and/or caregivers on the preparation and administration of DUPIXENT prior to use.
Footnotes
a Moderate-to-severe AD in patients aged 12+ years; severe AD in patients aged 6 months to 11 years.1
Abbreviations
AD, atopic dermatitis; Q2W, once every 2 weeks; Q4W, once every 4 weeks.
References
-
DUPIXENT Summary of Product Characteristics, 11/2025.
-
Derakhshandeh R et al. Expert Opin Drug Deliv 2025;22(5):747-756.
Summary
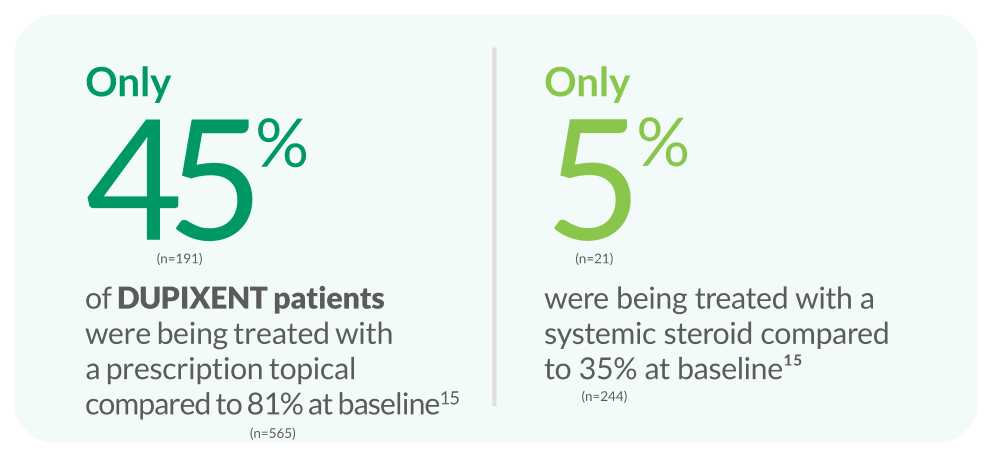
Of the 698 patients who initiated dupilumab and completed the baseline assessment, 425 (60.9%) completed the questionnaire at 30–36 months.
DUPIXENT ALLOWS PATIENTS TO BE TAPERED OFF OF STEROIDS
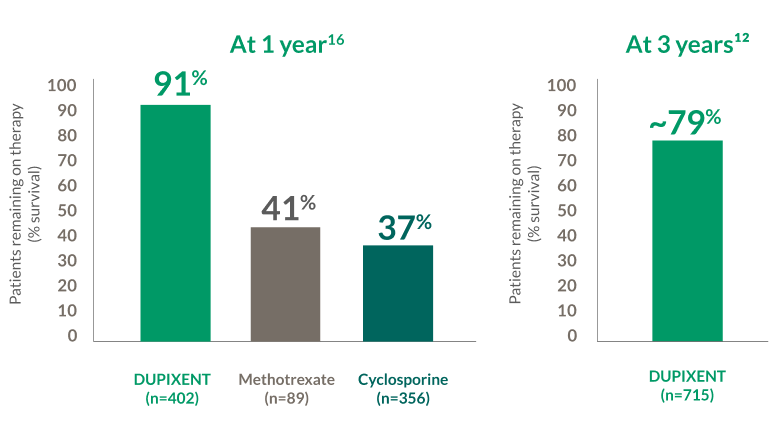
At 3 years WITH DUPIXENT
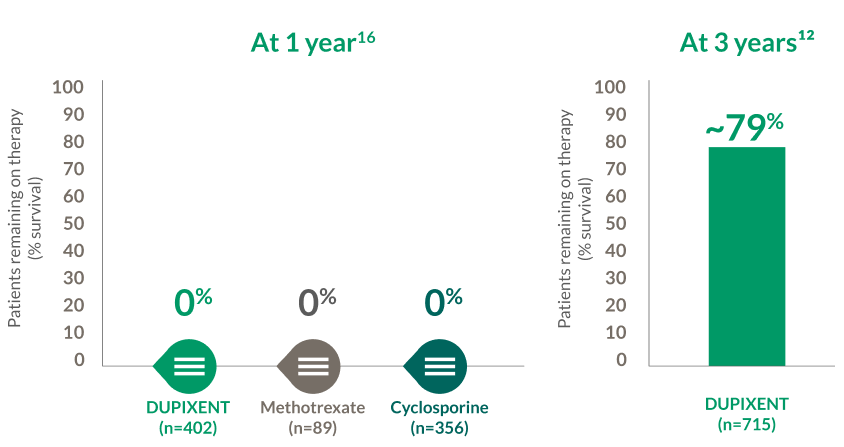
BIODAY REGISTRYe 18+ YEARS
~79% of patients with AD remained on DUPIXENT at 3 years12,f
BIODAY REGISTRYe 18+ YEARS
~79% of patients with AD remained on DUPIXENT at 3 years12,f
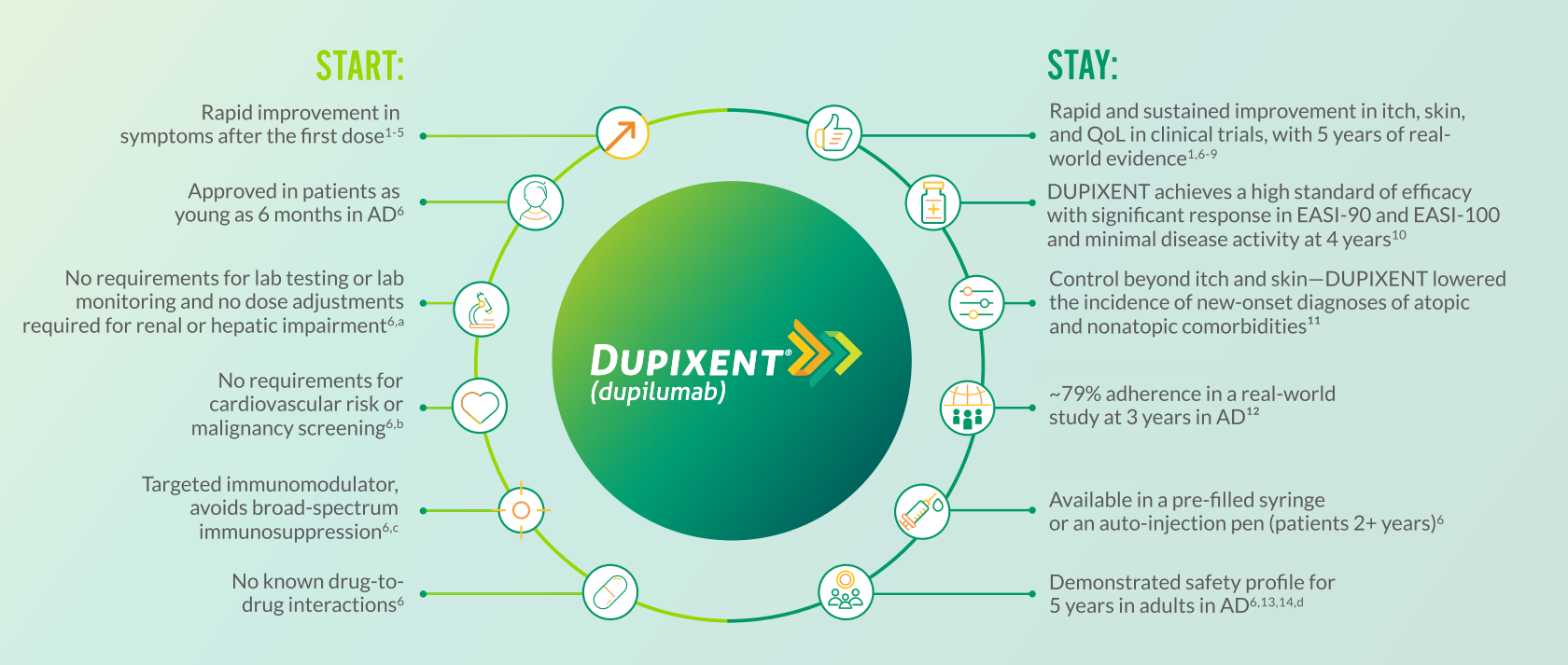
TARGET TYPE 2 INFLAMMATION IN AD EARLY WITH DUPIXENT FOR RAPID AND SUSTAINED RESULTS, AND CONTROL BEYOND ITCH AND SKIN
WHEN TOPICALS ARE NOT ENOUGH IN ATOPIC DERMATITIS

ONE TARGET, DUAL ACTION
DUPIXENT targets type 2 inflammation with dual inhibition of IL-4 and IL-13, improving itch, skin lesions, skin barrier function, and QoL6,17

SUSTAINED CONTROL FROM THE FIRST DOSE
DUPIXENT can help deliver control beyond itch and skin, with itch relief after the first dose, and sustained response in itch, skin, and QoL in clinical trials and the real-world setting1,6,18

START AND STAY WITH CONSISTENT SAFETY
DUPIXENT has a demonstrated long-term safety profile across 5 years as seen in an open-label extension trial14

CHOICE FOR ADULTS AND CHILDREN WITH ATOPIC DERMATITIS
for rapid and sustained results, and control beyond itch and skin1,2,6,19
Footnotes
a As demonstrated for up to 3 years in the open-label extension study.
b Based on the Pharmacovigilance Risk Assessment Committee recommendations.
c DUPIXENT is not an immunosuppressant.6,20
d In adults only.
e The BioDay registry is a prospective multicenter registry that contains daily practice data on the effectiveness and safety of DUPIXENT for the treatment of AD.12,16
f Includes topical medications, systemic steroids, and systemic immunosuppressants.12
Abbreviations
AD, atopic dermatitis; EASI, Eczema Area and Severity Index; IL, interleukin; QoL, quality of life.
References
-
Blauvelt A et al. Lancet. 2017;389(10086):2287-2303.
-
Blauvelt A et al. Lancet. 2017;389(10086):2287-2303 [suppl.].
-
Simpson EL et al. JAMA Dermatol. 2020;156(1):44-56.
-
Paller AS et al. Adv Ther. 2024;41(3):1046-1061.
-
Paller AS et al. J Am Acad Dermatol. 2020;83(5):1282-1293.
-
DUPIXENT Summary of Product Characteristics, 11/2025.
-
Blauvelt A et al. Am J Clin Dermatol. 2022;23(3):365-383.
-
Cork MJ et al. Dermatol Ther (Heidelb). 2023;13(11):2697-2719.
-
Boesjes CM et al. JAMA Dermatol. 2024;160(10):1044-1055.
-
Ferrucci S et al. Clin Exp Dermatol. 2024;49(12):1561-1572.
-
Tsai SYC et al. Allergy. 2024;79(10):2748-2758.
-
Spekhorst LS et al. JAMA Dermatol. 2022;158(9):1048-1056.
-
Beck LA et al. Am J Clin Dermatol. 2022;23(3):393-408.
-
Beck LA et al. JAMA Dermatol. 2024;160(8):805-812.
-
Kimball AB et al. Dermatol Ther (Heidelb). 2023;13(9):2107-2120.
-
Spekhorst LS et al. Allergy. 2020;75(9):2376-2379.
-
Weidinger S et al. Nat Rev Dis Primers. 2018;4(1):1.
-
Silverberg JI et al. Acta Derm Venereol. 2021;101(11):adv00585.
-
Paller AS et al. Lancet. 2022;400(10356):908-919.
-
Gandhi NA et al. Nat Rev Drug Discov. 2016;15(1):35-50.

© 2025 Sanofi and Regeneron Pharmaceuticals, Inc. All Rights Reserved. MAT-SE-2600351
SE-FILMEN-HÄR
