PCSK9 inhibitor treatment and outcomes

PCSK9i mAb therapy use was associated with a lower rate of ischaemic events and mortality rates vs. no PCSK9i* in a study of over 19,000 ASCVD patients without prior ischaemic events.1
Discover the findings from the methodologically advanced+ real-world OPTIMUS-CLASS study, part of the broader OPTIMUS (Outcomes and PrevenTlon Programme with PCSK9i Monoclonal Antibodies in ASCVD PopUlation without Prior ISchaemic Events) programme.1,2

Patients with ASCVD but no history of an ischaemic event who initiated a PCSK9i mAb‡ saw a:
30.9% 5-year relative risk reduction in ischaemic events and all-cause mortality vs. no PCSK9i* P<0.0001 (ARR 7.8%).1

- All patients with ASCVD are at very high or extreme risk of a potentially fatal CV event3
- LDL-C is the primary target for CV risk reduction and PCSK9 inhibitors can reduce LDL-C levels when used alone or in combination with statins3,4
- While clinical trials have established the effectiveness of PCSK9i mAbs across the different stages of ASCVD, real-world data remain limited1
- The OPTIMUS-CLASS study provides real-world evidence on the 5-year impact of PCSK9i mAbs‡ on ischaemic events and all-cause mortality in ASCVD patients without any prior ischaemic events1


The baseline characteristics for the PCSK9i mAb‡ group and no PCSK9i* group were well balanced.1
PCSK9i mAb‡
|
No PCSK9i*
|
Total
|
|
| Male (%) | 50.8 | 50.7 | 50.7 |
| Age | |||
| 18-44 | 1.3 | 1.7 | 1.6 |
| 45-64 | 30.7 | 30.8 | 30.8 |
| 65+ | 68.0 | 67.5 | 67.6 |
| Insurance | |||
| - Medicare Advantage¥ | 68.1 | 69.8 | 69.3 |
| - Commercial | 31.9 | 30.2 | 30.7 |
Adapted from Bhatt et al. 2026.
PCSK9i mAb‡
|
No PCSK9i*
|
Total
|
|
| Coronary Conditions | 76.7 | 76.0 | 76.1 |
| - Stable Angina | 74.7 | 73.5 | 73.8 |
| - Other IHD | 17.3 | 17.2 | 17.2 |
| - Prior Revascularisation | 25.6 | 25.5 | 25.5 |
| - PCI | 16.7 | 16.4 | 16.5 |
| - CABG | 12.0 | 11.9 | 11.9 |
| Ischaemic cerebrovascular disease | 9.4 | 9.6 | 9.6 |
| Peripheral artery disease | 19.1 | 19.4 | 19.3 |
| - Lower extremities | 3.9 | 4.1 | 4.0 |
| - Aorta | 4.9 | 4.9 | 4.9 |
| - OtherII | 10.3 | 10.4 | 10.4 |
Adapted from Bhatt et al. 2026.
PCSK9i mAb‡
|
No PCSK9i*
|
Total
|
|
| Diabetes | 35.9 | 35.8 | 35.9 |
| - No insulin | 23.9 | 23.8 | 23.9 |
| - On insulin | 12.0 | 12.0 | 12.0 |
| Hypertension | 79.5 | 79.5 | 79.5 |
| Liver disease | 5.1 | 5.2 | 5.2 |
| COPD | 9.9 | 9.9 | 9.9 |
| Heart failure | 8.7 | 8.5 | 8.6 |
| Chronic kidney disease | 10.7 | 10.4 | 10.4 |
| - Stage III | 9.2 | 8.9 | 8.9 |
| - Stage IV¶ | 1.5 | 1.5 | 1.5 |
| Atrial fibrillation | 9.7 | 9.7 | 9.7 |
| Tobacco use | 17.6 | 17.7 | 17.6 |
| Cancer | 11.9 | 11.3 | 11.4 |
| - Diagnosis | 8.9 | 9.0 | 8.9 |
| - Medication | 4.8 | 4.6 | 4.6 |
Adapted from Bhatt et al. 2026.
PCSK9i mAb‡
|
No PCSK9i*
|
Total
|
|
| LLT use during 1-year prior to index, % | |||
| Any statin use | 61.0 | 61.6 | 61.4 |
| - Low-intensity | 5.5 | 6.5 | 6.2 |
| - Moderate-intensity | 23.8 | 25.9 | 25.3 |
| - High-intensity | 31.7 | 29.3 | 29.9 |
| Ezetimibe | 33.4 | 33.3 | 33.3 |
| Ezetimibe w/o statin | 11.3 | 11.0 | 11.1 |
| Icosapent ethyl | 3.1 | 3.0 | 3.0 |
| Bempedoic acid | 0.4 | 0.5 | 0.5 |
| Any statin, ezetimibe or bempedoic acid | 72.4 | 72.7 | 72.6 |
| Other CV SOC during 1-year prior to Index, % | |||
| Beta-blockers | 52.6 | 52.3 | 52.4 |
| ACEi / ARB | 58.2 | 58.1 | 58.1 |
| Antiplatelets** | 23.8 | 23.5 | 23.6 |
| Anticoagulants | 10.5 | 10.5 | 10.5 |
Adapted from Bhatt et al. 2026.
PCSK9i mAb‡
|
No PCSK9i*
|
Total
|
|
| Mean (SD), mmol/L | 3.0 (1.1) | 3.0 (1.1) | 3.0 (1.1) |
| Mean (SD), mg/dL | 117.8 (42.0) | 116.1 (43.2) | 116.5 (42.9) |
| Median, mmol/L | 3.1 | 2.9 | 2.9 |
| Median, mg/dL | 118.0 | 112.0 | 113.0 |
Adapted from Bhatt et al. 2026.

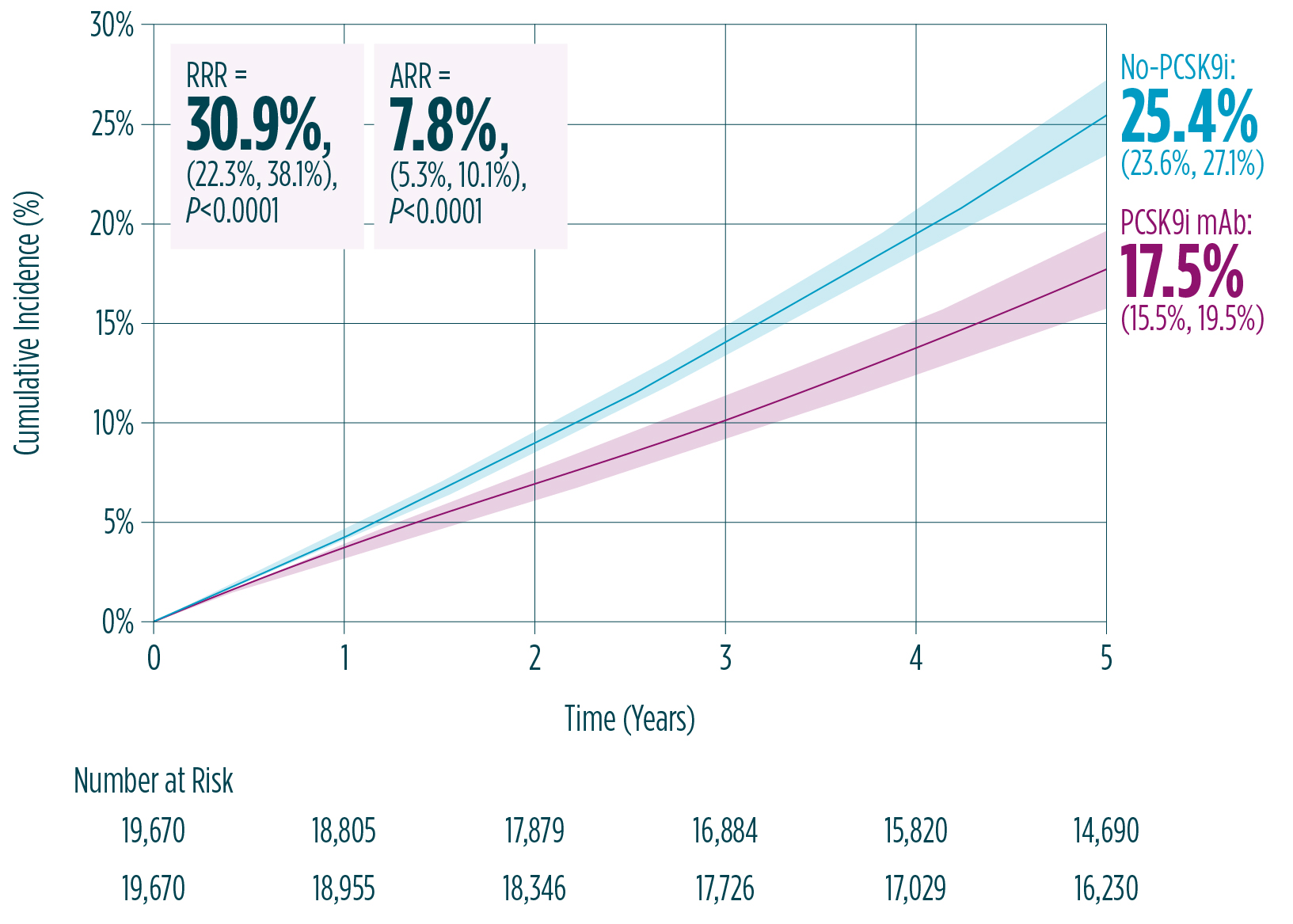
PCSK9i mAb‡ treatment was associated with a 30.9% relative reduction in the risk of nonfatal MI, nonfatal IS or all-cause mortality in ASCVD patients without a prior ischaemic event.1
The estimated 5-year event rate for the composite endpoint of nonfatal MI, nonfatal IS or all-cause mortality was significantly lower in the PCSK9i mAb‡ group vs. the no PCSK9i* group.1
The 5-year event rate was 17.5% (95% CI 15.5, 19.5) in the PCSK9i mAb‡ group (n=6,545) vs. 25.4% (95% CI 23.6, 27.1) in the no PCSK9i* group (n=13,125), resulting in a significant 30.9% relative reduction in the risk of first MACE (ARR 7.8%) (P<0.0001).1
Estimated event rates over time for the primary endpoint with parametric G-formula (ITT)1
A reduction in 5-year event rate was also seen in the PCSK9i mAb‡ group across each individual endpoint, with 28.3%, 26.4% and 28.5% RRR observed across nonfatal MI, nonfatal IS and all-cause mortality event rates, respectively, vs. the no PCSK9i* group.5
Individual endpoint 5-year event rates (ITT)5
PCSK9i mAb‡
|
No PCSK9i*
|
RRR
|
ARR
|
|
| Nonfatal MI | 5.2 (4.3, 6.3) | 7.3 (6.6, 8.1) | 28.3 (12.0, 40.6
[P<0.0001]) |
2.1 (0.8, 3.1
[P<0.0001]) |
| Nonfatal IS | 4.0 (3.1,4.7) | 5.4 (4.6, 6.3) | 26.4 (6.5, 45.7
[P=0.02]) |
1.5 (0.3, 2.7
[P=0.02]) |
| All-cause mortality | 8.7 (7.5, 9.8) | 12.2 (11.2, 13.0) | 28.5 (16.6, 39.1
[P<0.0001]) |
3.5 (2.0, 4.9
[P<0.0001]) |
Adapted from Bhatt et al. 2026. Supplementary Material.
In the ITT population, patients in the PCSK9i mAb‡ group went from an LDL-C level of 117.8 mg/dL to 78.0 mg/dL at follow-up after 5 years.1 This resulted in a 39.8 mg/dL absolute reduction in LDL-C, representing a 33.8% percentage reduction.1 These findings are consistent with the CTT††, which demonstrated a strong association between RRR in MACE per 1 mmol/L reduction in LDL-C.6
Relationship between LDL-C reduction and relative risk reduction in ischaemic events compared to CTT meta-analysis1
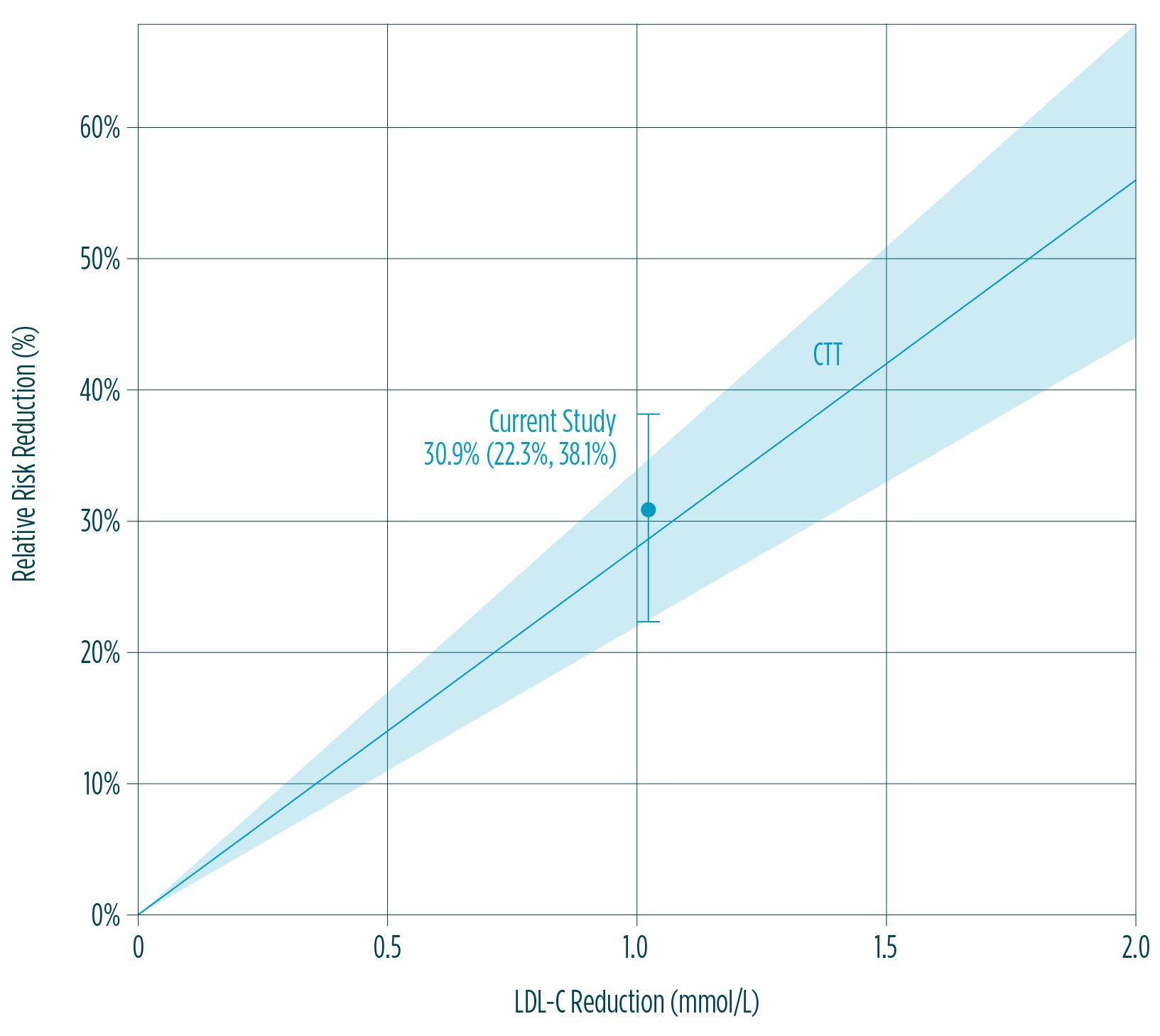
When looking at patients who were treated with or without statins, both the with statins and without statins PCSK9i mAb‡ groups had lower cumulative event rates than their equivalent no PCSK9i* groups.5 Current study 30.9% (95% CI 22.3%, 38.1), CTT RRR 28.8% (95% CI 22.6%, 35.0%)
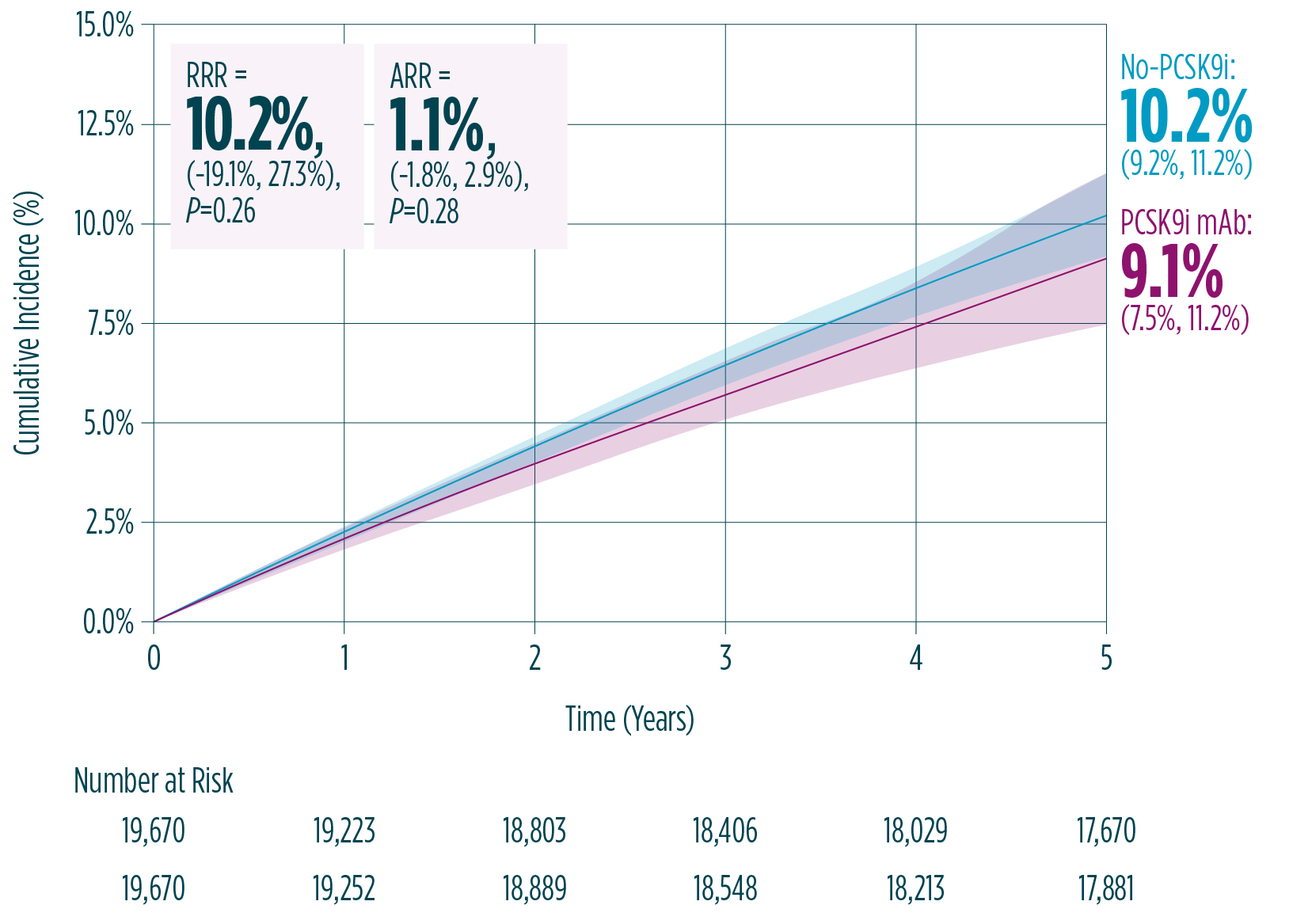
The falsification analysis, used to support the validity of data, found no significant difference between the PCSK9i mAb‡ and no PCSK9i* groups.1
To help determine whether the lower rate of MACE with PCSK9i mAbs‡ VS. no PCSK9i* was confounded by other factors, the study assessed whether PCSK9i mAbs‡ vs. no PCSK9i* was associated with any unexpected benefit in the falsification endpoint, defined as composite of cancer, hospitalised major bleeding or hospitalised sepsis.1 At 5 years, the incidence of the falsification endpoint was similar in the PCSK9i mAbs‡ group (9.1%) and no PCSK9i* group (10.2%), supporting the validity of the MACE data.1
Falsification analysis1
In ASCVD patients without prior ischaemic events, PCSK9i mAb‡ therapy compared with no PCSK9i* treatment was associated with a relative reduction in the risk of ischaemic events or mortality.1
*No PCSK9i represents no PCSK9 monoclonal antibodies (alirocumab or evolocumab) or PCSK9 small interfering RNA (inclisiran).1
+RWE studies can vary substantially in their methodological approaches, which may contribute to heterogeneity or unexpected findings across analyses. Ensuring that key epidemiological principles – such as appropriate time zero definition, new user design considerations, handling of open claims data, and assessment of potential time related biases – are rigorously applied remains essential to generate reliable insights. High quality RWE therefore depends on robust and methodically advanced approaches such as propensity score matching and G-computation used in the study.
‡PCSK9i mAb represents alirocumab or evolocumab.1
¥A claims database, representing an insured population in the US.1
§Represents health plan in the US offered by a private company that contracts with Medicare to provide patients with hospital and medical insurance benefits.1
||Includes any type of disease that is non-coronary, non-cerebrovascular, or does not involve the lower extremities or aorta.1
¶Includes dialysis or renal transplant.1
**Includes clopidogrel, ticagrelor, and prasugrel; 98.8% use in this category was for these agents. Additional agents were anagrelide, cilostazol, dipyridamole (including aspirin combo), pentoxifylline and vorapaxar sulphate.1
++CTT relative risk reduction = 28% (95% CI 22, 34) per mmol/L reduction in LDL-C.1
PRALUENT® (alirokumab), injektionsvätska, lösning i förfyllda injektionspennor 75 mg, 150 mg och 300 mg, Rx, F*, ATC-kod C10AX14. Indikation: PRALUENT är indicerat hos vuxna med primär hyperkolesterolemi (heterozygot familjär samt icke-familjär) eller blandad dyslipidemi och hos pediatriska patienter 8 år och äldre med heterozygot familjär hyperkolesterolemi, som tillägg till diet samt hos vuxna med etablerad aterosklerotisk kardiovaskulär sjukdom för att reducera kardiovaskulär risk genom att sänka nivåerna av LDL-kolesterol, i tillägg till korrigering av andra riskfaktorer. PRALUENT ges i kombination med maximalt tolererad statindos med eller utan annan lipidsänkande behandling, ensamt eller i kombination med annan lipidsänkande behandling hos patienter som är statinintoleranta, eller där statinbehandling är kontraindicerad. Varning och försiktighet: PRALUENT ska användas med försiktighet till patienter med gravt nedsatt njur- och leverfunktion. För ytterligare information, se www.fass.se. Kontaktuppgifter: PRALUENT tillhandahålls av Sanofi AB, tel +46 8 634 50 00, www.sanofi.se. Vid frågor om våra läkemedel kontakta: infoavd@sanofi.com. Datum för senaste översyn av produktresumé: oktober 2025.
*Begränsningar: Subventioneras för patienter med diagnostiserad heterozygot familjär hyperkolesterolemi som trots maximal tolererbar behandling med statin och ezetimib har kvarstående LDL-kolesterol på 2,6 mmol/L eller högre. Subventioneras för patienter med diagnostiserad aterosklerotisk hjärt- och kärlsjukdom som trots maximal tolererbar behandling med statin och ezetimib har kvarstående LDL-kolesterol på 1,8 mmol/L eller högre. Subventioneras för patienter med diagnostiserad diabetes mellitus och målorganskada (mikroalbuminuri, retinopati eller neuropati), eller minst tre viktiga riskfaktorer, eller tidig debut av typ 1 diabetes mellitus med lång duration, som trots maximal tolererbar behandling med statin och ezetimib har kvarstående LDL-kolesterol på 2,6 mmol/l eller högre.
ACEi = angiotensin convertase enzyme inhibitor; AE = adverse event; ARB = angiotensin receptor blocker; ARR = absolute risk reduction; ASCVD = atherosclerotic cardiovascular disease; CABG = coronary artery bypass graft; CI = confidence interval; COPD = chronic obstructive pulmonary disease; CTT = Cholesterol Treatment Trialists' Collaboration; CV = cardiovascular; HeFH = heterozygous familial hypercholesterolaemia; HIS = high-intensity atorvastatin; IHD = ischaemic heart disease; IS = ischaemic stroke; ITT = intention-to-treat; LDL-C = low-density lipoprotein cholesterol; LLT = lipid-lowering therapy; mAb = monoclonal antibody; MACE = major adverse cardiovascular event; MI = myocardial infarction; PCI = percutaneous coronary intervention; PCSK9 = proprotein convertase subtilisin/ kexin type 9; PCSK9i = proprotein convertase subtilisin/kexin type 9 inhibitor; RNA = ribonucleic acid; RRR = relative risk reduction; RWE = real-world evidence; SD = standard deviation; SOC = standard of care.
-
Bhatt DL, Perrone Filardi P, Khan I, et al. PCSK9 inhibitor treatment and outcomes in patients with atherosclerotic cardiovascular disease but without prior ischaemic events: an observational study. Eur Heart J. 2026;ehag176.
-
Naimi Al, Cole SR and Kennedy EH. An introduction to g methods. Int J Epidemiol. 2017;46(2):756-762.
-
Mach F, Koskinas KC, Roeters van Lennep JE, et al. 2025 Focused Update of the 2019 ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J. 2025;46(42):4359-4378.
-
Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med. 2018;379(22):2097-2107.
-
Bhatt DL, Perrone Filardi P, Khan I, et al. PCSK9 inhibitor treatment and outcomes in patients with atherosclerotic cardiovascular disease but without prior ischaemic events: an observational study. Eur Heart J. 2026;ehag176. Supplementary material.
-
Cholesterol Treatment Trialists' Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-1681.
-
PRALUENT (alirocumab) Summary of Product Characteristics. Paris, France: sanofi-aventis groupe Oct 2025.
Relaterade Artiklar
What is PRALUENT®(alirocumab)?
PRALUENT®: a PCSK9i that ticks all the boxes1–4
PRALUENT is a PCSK9i that reduces the levels of LDL-C in the blood.2 It is a fully human IgG1 monoclonal antibody that works by inhibiting the binding of PCSK9 to LDL- receptors. As a result, PRALUENT increases the number of LDL-receptors available to clear LDL, thereby lowering LDL-C levels.2 Elevated LDL-C levels have been significantly associated with cardiovascular disease such as heart attacks and strokes.1
Why choose PRALUENT®?
The usual starting dose for PRALUENT is 75 mg administered subcutaneously once every 2 weeks. Patients requiring larger LDL-C reduction (>60%) may be started on 150 mg once every 2 weeks, or 300 mg once every 4 weeks (monthly), administered subcutaneously.2
SE-FILMEN-HÄR
